
Executive Summary
- Most healthcare organizations fail at execution, not strategy.
- Most execution fails because of the quality of the field force people, where the rubber hits the road.
- Traditional Sales Force Effectiveness (SFE) tools track activity but don’t drive intrinsic motivation.
- The MAP Framework (Purpose → Mastery → Autonomy) bridges this gap.
- This article provides concrete tactics for each pillar, not just theory.
- Success stories from pharma are used illustratively, not as definitive case studies.
This is a 2026 AI-enabled adaptation of an article that I wrote in 2014 based on the work of Daniel Pink and Simon Sinek – https://www.linkedin.com/pulse/20140707021108-3531167-understanding-significance-of-mastery-autonomy-and-purpose-in-field-force-excellence/

The Real Problem Isn’t Strategy—It’s Execution
Every healthcare organization struggles to continuously upskill and deploy its field force. Without an effective field force, companies miss commercial goals or resort to aggressive tactics that invite regulatory scrutiny.
Marketing teams often craft robust product strategies. They get the science, positioning, and messaging right. Yet implementation is where most companies lose traction.
Why?
Strategy design is a centralised, reflective process managed by a few. Implementation is a highly decentralised task executed by thousands of medical representatives (MRs) daily. While a strategy remains stable on paper, its execution must constantly adapt to the real-time abilities, motivation, and constraints of the frontline.

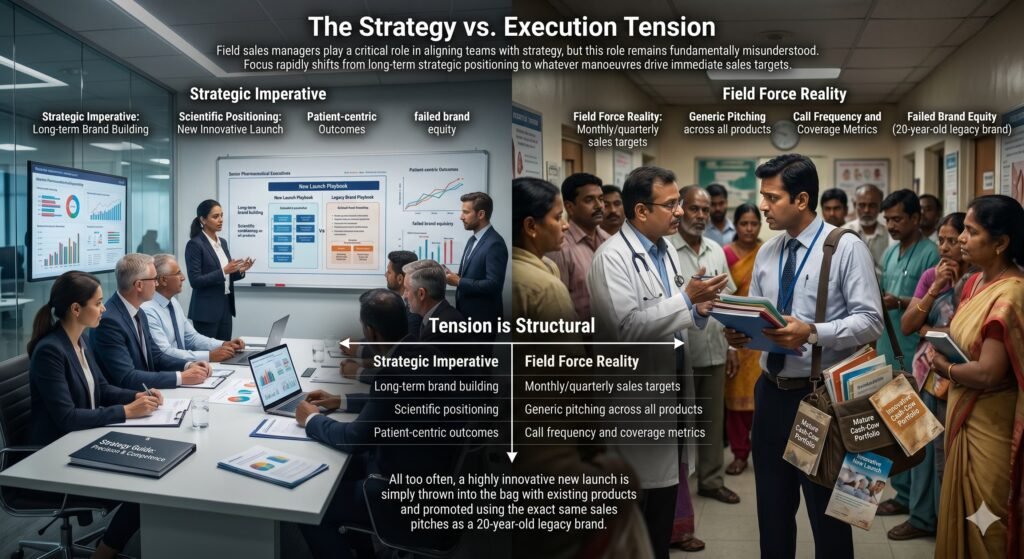
The Strategy vs. Execution Tension
Field sales managers play a critical role in aligning teams with strategy, but this role remains fundamentally misunderstood. Given the multiple tactical tasks an MR handles daily, focus rapidly shifts from long-term strategic positioning to whatever maneuvers drive immediate sales targets.
The tension is structural:
| Strategic Imperative | Field Force Reality |
|---|---|
| Long-term brand building | Monthly/quarterly sales targets |
| Scientific positioning | Generic pitching across all products |
| Patient-centric outcomes | Call frequency and coverage metrics |
All too often, a highly innovative new launch is simply thrown into the bag with existing products and promoted using the exact same sales pitches as a 20-year-old legacy brand.
An effective field force clearly distinguishes between maintaining a mature cash-cow portfolio and executing precise, scientific positioning for a new launch. This requires a level of competence and intrinsic motivation that traditional field forces rarely possess. The result: suboptimal market penetration and failed brand equity.
The Modern Blueprint for Success
Breaking through the noise to build sustainable, multi-crore mega-brands is rare. When it happens—for example, in the successful expansion of certain Indian pharma companies into chronic cardiac care or the commercial deployment of novel metabolic molecules—the differentiator is never just the molecule. It is clear strategy combined with solid execution.
Note on examples: The following company references are for illustrative purposes only, based on observable market outcomes, not confirmed internal adoption of the MAP framework.
What is remarkable across successful companies is the diversity of their approaches. Yet universally, their success relies on the field force faithfully translating marketing strategy into clinical value during interactions with healthcare professionals (HCPs).
The synergy between strategy creators and executors creates market leaders. They succeed not just by tracking their people, but by making everyday work deeply meaningful, clinically engaging, and personally rewarding.
Moving Beyond Pure SFE: The MAP Framework
Crucially, frontline professionals must be selected and developed not just for qualifications, but for mindset. The modern environment demands a field force that can operate effectively without constant, over-the-shoulder supervision.
With physicians restricting physical access to seconds, and digital channels flooding their feeds, the MR’s job has become highly autonomous. Top-tier professionals thrive on this independence.
This brings us to the core of intrinsic motivation—Purpose, Mastery, and Autonomy—grounded in Deci & Ryan’s Self-Determination Theory and popularized by Daniel Pink. When applied to commercial execution, I call this the MAP Framework:
[ PURPOSE ]
(The "Why")
│
▼
[ MASTERY ]
(The "How")
│
▼
[ AUTONOMY ]
(The "What")All three elements are non-negotiable to build resilience. MAP allows a field representative to see the big picture and systematically implement strategies even without daily management oversight.
Modern SFE tools, AI-driven CRM platforms, and geo-tracking systems are useful for aligning activities. But SFE is an external regulator; MAP is an internal driver.
To be clear: Good SFE already incorporates behavioral drivers. The point is not to dismiss SFE but to add the explicit layer of intrinsic motivation that tools alone cannot create.
When SFE metrics are combined with MAP, they create a powerful connection between what the organisation needs to achieve and what the individual finds professionally meaningful.
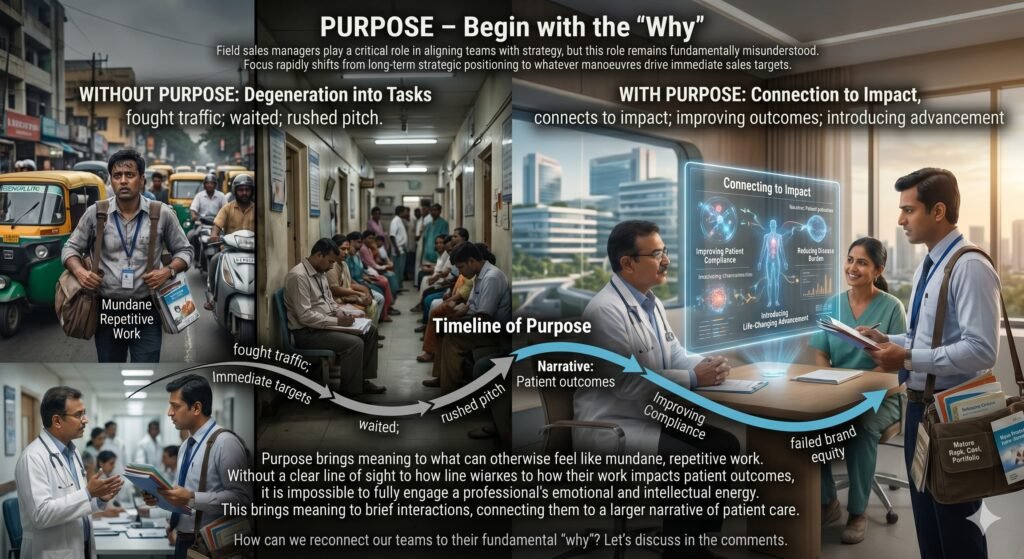
1. Purpose – Begin with the ‘Why’
Without a clear line of sight to how their work impacts patient outcomes, it is impossible to fully engage a professional’s emotional and intellectual energy. Purpose brings meaning to what can otherwise feel like mundane, repetitive work.
Without purpose, a representative’s day degenerates into: fighting traffic, waiting in clinic corridors, delivering a rushed pitch to a distracted doctor. With purpose, that brief interaction connects to a larger narrative: improving patient compliance, reducing disease burden, or introducing a life-changing therapeutic advancement.
✅ Concrete Tactic: The 5-Minute Patient Story
Action: Start every monthly sales meeting with one real patient story (anonymized and compliant). Not a data slide. A story.
Example: “Mrs. Sharma, 58, with uncontrolled diabetes for 7 years. Her doctor was hesitant to escalate therapy until our rep shared the new cardiovascular outcome data. Three months later, her HbA1c dropped from 9.2 to 7.1.”
Why it works: Purpose cannot be taught in a training module. It must be felt. Stories create emotional anchors that outlast any incentive plan.
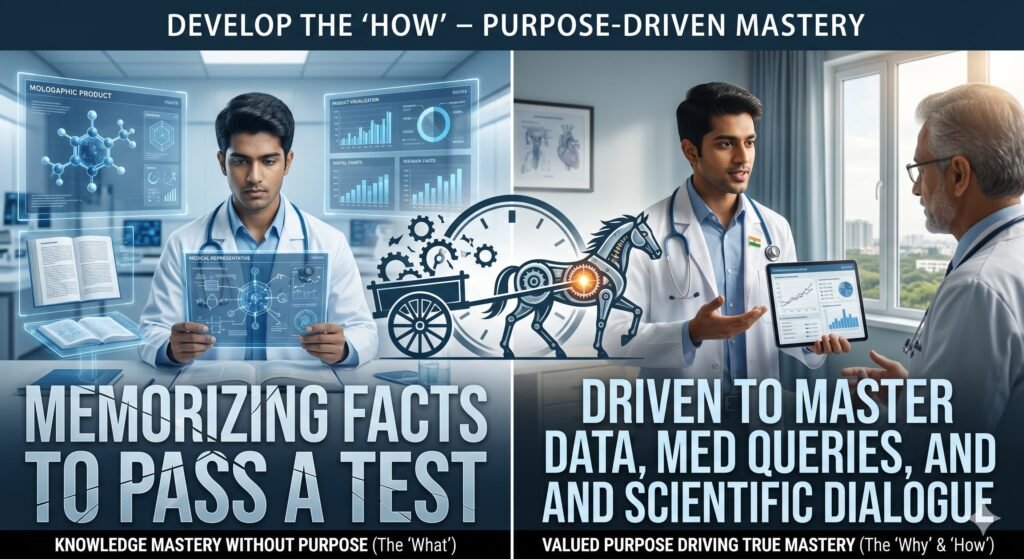
2. Mastery – Develop the ‘How’
Progressive companies spend significant resources on product knowledge, disease-state expertise, and digital tools. However, emphasizing mastery without first establishing purpose puts the cart before the horse.
Unless a professional understands the purpose of their execution, they lack the internal drive to achieve true mastery. They simply memorise facts to pass a test.
Conversely, a representative who deeply values the purpose of a molecule will actively invest effort to master clinical data, navigate complex medical queries, and conduct peer-level scientific dialogues with specialists.
✅ Concrete Tactic: Clinical Case Debates (Not Product Tests)
Action: Replace quarterly product knowledge tests with 90-minute clinical case debates in small groups.
Format: Present a real de-identified patient case. Two teams argue different therapeutic approaches using your product portfolio. A medical affairs moderator scores clinical reasoning, not product promotion.
Example: “55-year-old with newly diagnosed hypertension, mild CKD, and gout. Which pathway do you prioritize, and why?”
Why it works: Mastery in the modern era is not recall—it is clinical reasoning under uncertainty. Debates build that skill and are intrinsically motivating.

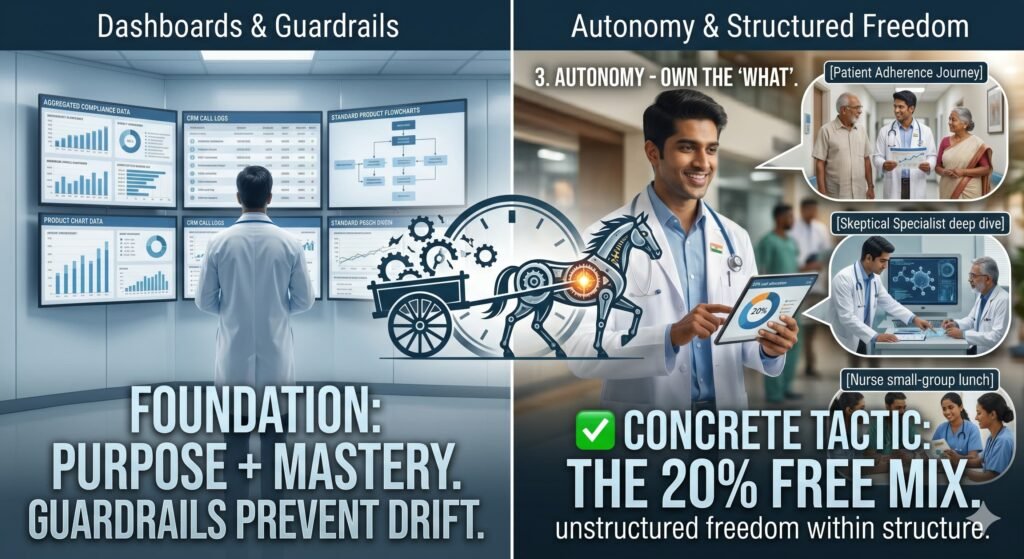
3. Autonomy – Own the ‘What’
Nobody likes to be micro-managed by a dashboard. But autonomy without mastery is dangerous—it leads to strategic drift, off-label messaging, and compliance failures.
When built upon a foundation of Purpose and Mastery, Autonomy empowers the field force. It gives them flexibility to tailor their omnichannel approach, balance digital detailing with in-person relationship building, and act as agile problem-solvers.
✅ Concrete Tactic: The 20% Free Mix
Action: Allow each MR to allocate 20% of their weekly call mix to activities not in the standard CRM playbook—provided they can justify the clinical or relationship rationale.
Examples:
- Accompanying a patient to understand the adherence journey
- Organizing a small-group lunch with a nurse educator (non-promotional)
- Spending an extra hour with a skeptical specialist to address deep scientific questions
Governance: Require a brief (3-sentence) monthly reflection: What did you try? What did you learn? What patient or HCP outcome improved?
Why it works: Autonomy without accountability is chaos. The 20% rule creates structured freedom. It signals trust while demanding intentionality.
The Internal Compass
An excellent field force understands its core purpose, possesses the mastery to deliver clinical value, and is trusted with the autonomy to execute dynamically.
MAP serves as an internal compass that keeps the frontline moving in the right direction—completely independent of algorithmic tracking or top-down directives.
| If you focus only on… | You get… |
|---|---|
| SFE tools + targets | Compliant activity, not committed performance |
| Purpose alone | Enthusiasm without competence |
| Mastery alone | Highly skilled reps who don’t know why it matters |
| Autonomy alone | Strategic drift and compliance risk |
| MAP together | Resilient, self-directed, clinically valuable field force |
Putting It Into Practice
To build a sustainable, future-ready commercial organization:
- Clear the path to Purpose – Start every meeting with a patient story, not a sales number.
- Coach and facilitate clinical Mastery – Replace product tests with case debates.
- Grant strategic Autonomy – Introduce the 20% Free Mix with structured reflection.
SFE tools will tell you where your reps went and what they detailed. MAP will tell you why they showed up and how well they thought on their feet.
One is a dashboard. The other is a compass.
You need both. But only one will work when the dashboard goes dark.

Disclaimer: Company examples cited are for illustrative purposes based on observable market outcomes and do not imply confirmed internal adoption of the MAP framework. Readers should verify the current UCPMP status with applicable regulatory authorities.





{kind=link}