
In 1989, oncology in India was not a business unit. It was a scientific outpost.
I entered this field when we measured success by the depth of a clinical conversation, not the breadth of a CRM dashboard. Today, oncology is a multi-billion-dollar strategic chess match. But as we have gained scale, there is a lingering question: have we lost the plot?
Looking back at four decades from the frontlines, the evolution of cancer care in India was not a slow climb. It was a series of radical rewiring events that changed how we think, sell, and treat.

1. The Era of the Monk-Marketer (The 1990s)
The Vibe: Scarcity and Science.
The Play: In the 90s, if you did not understand the Krebs cycle or the nuances of Adriamycin cardiotoxicity, you did not get past the chamber door. With fewer than 200 active medical oncologists nationwide, detailing as we know it today did not exist. You engaged in peer-level scientific discourse.
The Lesson: Credibility was the only currency. There were no digital decks or WhatsApp groups, just a briefcase full of trial data and the patience to wait three hours for a ten-minute window of brilliance.
2. The Democratization Disruptors (The 2000s)
The Vibe: Generic Aggression.
The Play: Indian Pharma did what it does best: it broke the monopoly. Domestic giants did not just enter oncology; they democratized it. By leveraging the 1970 Patents Act (which recognized process over product), they took life-saving molecules and turned them into volume plays. Landmark moments, such as the patent challenges surrounding Imatinib, signaled a new era.
The Shift: Access exploded. This was not because cancer rates suddenly changed, but because the price-gate was dismantled. Oncology moved from the elite metros to the masses.
3. The Institutional Capture (The 2010s)
The Vibe: The System Bends.
The Play: This was the uncomfortable decade. As the market became lucrative, power shifted from the clinician’s pen to the hospital’s procurement desk.
The Reality: Deep discounting and institutional margins became the primary levers of growth. Science often took a backseat to the commercial deal. Even the most compliant multinational corporations found themselves in a race to the bottom, trapped in a system of high trade margins they helped create but could no longer control.
4. Biological Industrialization (2015 to Present)
The Vibe: Complexity as a Moat.
The Play: Just as we risked total commoditization, biology struck back. With the rise of biosimilars—anchored by landmarks like the launch of Reditux (Rituximab)—India proved it could do more than just replicate chemistry. It could master the cell.
The New Frontier: We are now in the age of biomarker-led precision. We have moved from carpet-bombing cells to sniper-striking receptors. CAR-T and Immunotherapy are no longer futuristic slides; they are the current P&L drivers.
The Invisible Backbone: A Strategic Irony
Here is the truth no one likes to admit at sales conferences: The Old Guard—Doxorubicin, Cisplatin, and Cyclophosphamide—still carries the weight of Indian oncology.
They are the backbone of almost every protocol. They drive the volume. The irony? No one promotes them. The margins are gone. They are the invisible essential, while the industry’s spotlight and budget chase the one percent of patients who can afford the latest innovation.
Final Word: Are You Selling or Solving?
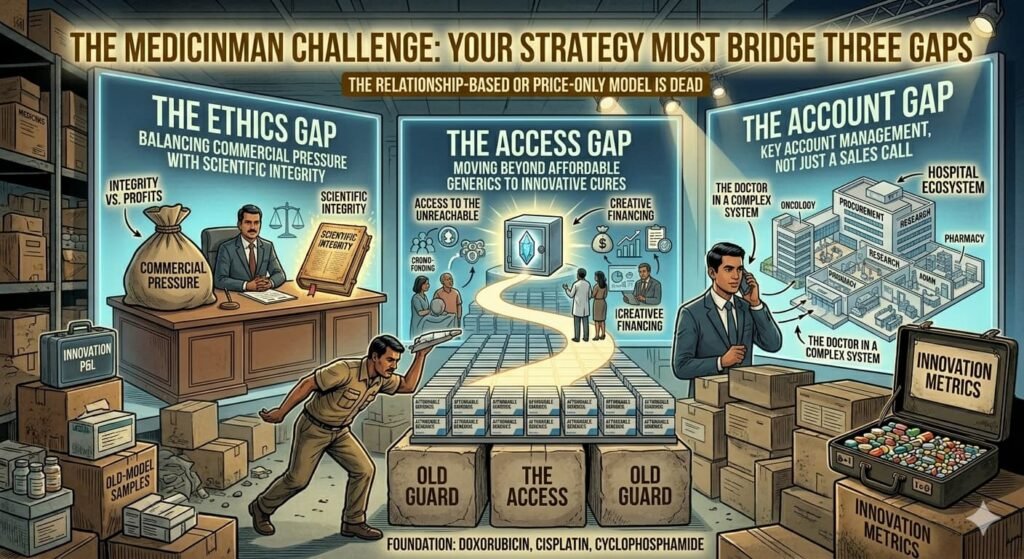
As we look toward the next decade, the relationship-based or price-only model is dead. To win in the new oncology landscape, your strategy must bridge three gaps:
- The Ethics Gap: Balancing commercial pressure with scientific integrity.
- The Access Gap: Moving beyond affordable generics to finding creative financing for innovative cures.
- The Account Gap: Realizing that the Doctor is now part of a complex Hospital Ecosystem that requires Key Account Management, not just a sales call.
I remember waiting for faxes and chasing physical journals.
Today, data is instant, and therapies are miraculous. But as we move from selling drugs to solving oncology, one thing remains unchanged:
If your strategy does not ultimately serve the patient sitting in the waiting room
it is not a strategy. It is just noise.
About the Author
Subroto Banerjee is a veteran pharmaceuticals executive with over three decades of experience, currently serving as President and Founding Team Member at Restory Healthytech Private Limited in Hyderabad, where he drives all business activities, stakeholder value growth, and brand building for healthy aging solutions.
His career highlights include leading India business as President at Strides Shasun Ltd (2012-2016), overseeing FDF and injectables (Agila prior to divestment), and roles at Dabur Pharma Ltd (2007-2010) as General Manager for generic oncology, Dr. Reddy’s Laboratories (2001-2007) directing oncology sales and marketing (including India’s first biosimilar Rituximab launch), Biological E Ltd (1999-2001), and Criticare Labs (1994-1999).
As an independent consultant since 2016, he focuses on pharma M&As, sales/marketing strategies, digital pharma shifts, and real-world evidence in oncology.
Sources:
Editor’s Note: To authenticate the claims made in this article, the following references and historical milestones provide the necessary background:
- The Patents Act of 1970: This was the foundational legislative move that allowed Indian companies to reverse-engineer molecules, leading to the democratization seen in the 2000s.
- Novartis v. Union of India (2013): The landmark Supreme Court case regarding the drug Glivec (Imatinib). This case is essential for understanding the shift in the 2000s regarding patent protection and the affordability of cancer drugs in India.
- Launch of Reditux (2007): Dr. Reddy’s launch of the world’s first biosimilar Rituximab. This serves as the anchor for Section 4, proving India’s early entry into complex biological manufacturing.
- National Cancer Grid (NCG) Data: For insights into how the Old Guard drugs (Cisplatin, etc.) remain the volume drivers in India, refer to the NCG’s standardized treatment guidelines which highlight the continued reliance on cytotoxic backbones in public health settings.
- NPPA Price Controls (2019): The National Pharmaceutical Pricing Authority’s move to cap trade margins on 42 non-scheduled anti-cancer drugs provides the legislative context for the commercial distortion discussed in Section 3.




{kind=link}