
The recent Mint Lounge analysis captured a striking consumer reality: pain relief in India is becoming a fast-moving consumer economy, powered by quick commerce, e-pharmacies, and the psychology of instant relief. Urban Indians are ordering pain balms, sleep gummies, and menstrual cramp patches with the same ease as groceries.
Reading that piece as a lifestyle trend is easy. Reading it as a healthcare professional is deeply unsettling.
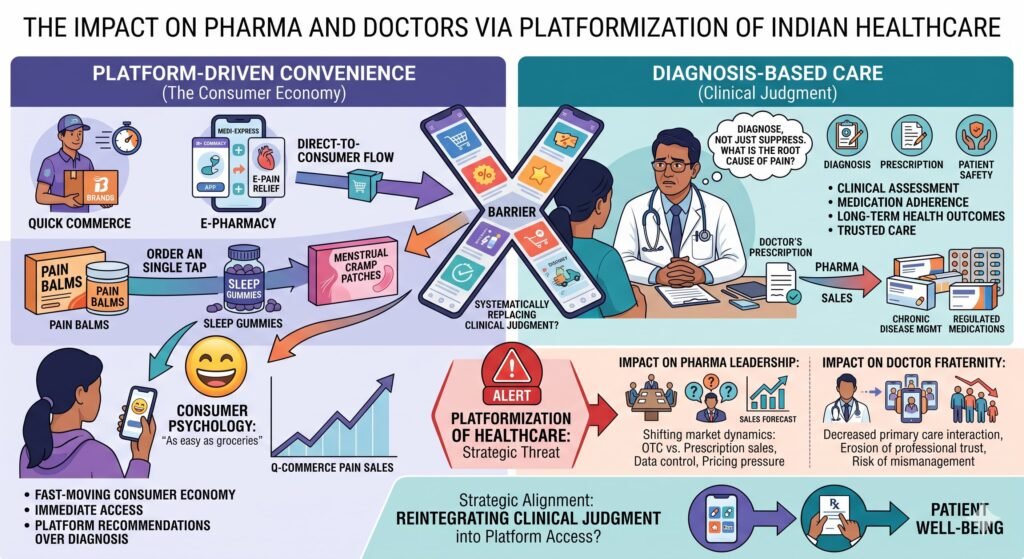
Because beneath the convenience lies a quieter, more disruptive question: Are e-pharmacies and quick-commerce platforms systematically replacing the clinical judgment of doctors? Are patients—without realizing it—drifting away from the very professionals trained to diagnose, not just suppress, their pain?
This is not a consumer story. This is the platformization of healthcare—and it represents the most urgent strategic threat assessment for pharma leadership and the medical fraternity in India today.
What the Mint Article Actually Reveals
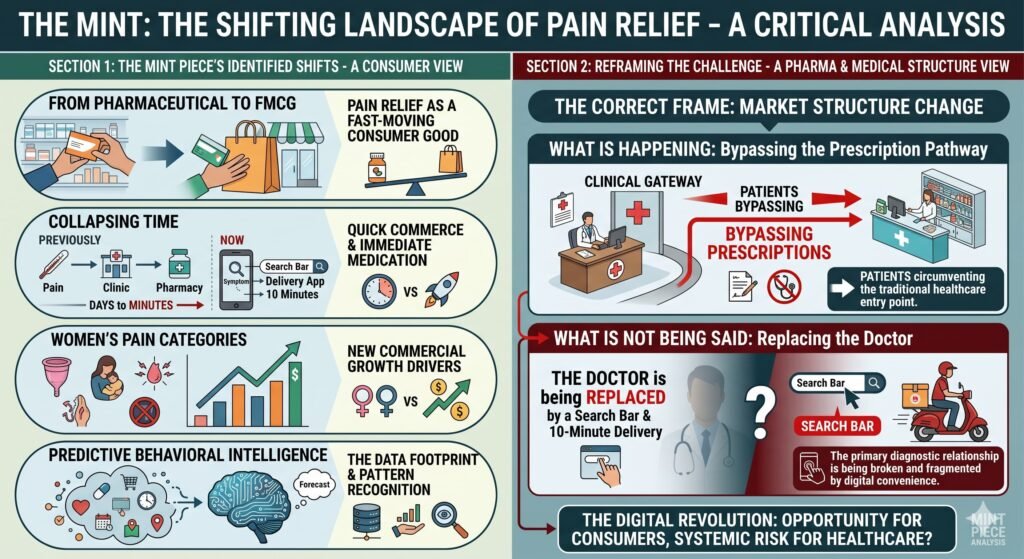
The Mint piece correctly identifies several shifts:
- Pain relief has moved from a pharmaceutical category to a fast-moving consumer good
- Quick commerce has collapsed the time between symptom and medication from days to minutes
- Women’s pain categories are becoming major commercial growth drivers
- The data footprint of pain-related purchases creates predictive behavioral intelligence
But for pharma companies and doctors, the correct frame is not consumer behaviour. It is a market structure change:
What is happening: Patients are bypassing the prescription pathway entirely.
What is not being said: The clinical gateway—the doctor—is being replaced by a search bar and a 10-minute delivery window.
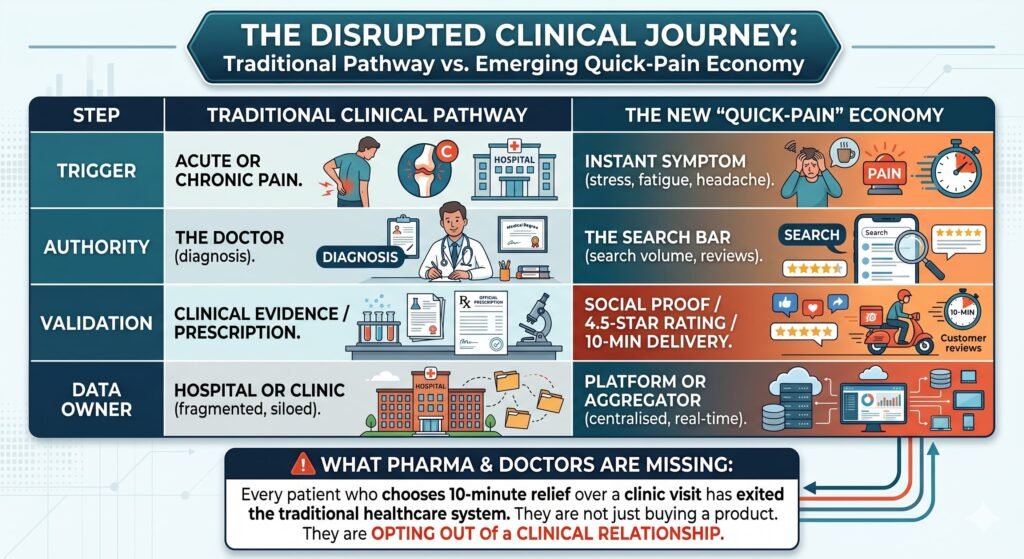
The Disrupted Clinical Journey
To understand the scale of this shift, compare the traditional pathway with the emerging “quick-pain” economy:
| Step | Traditional Clinical Pathway | The New “Quick-Pain” Economy |
|---|---|---|
| Trigger | Acute or chronic pain | Instant symptom (stress, fatigue, headache) |
| Authority | The doctor (diagnosis) | The search bar (search volume, reviews) |
| Validation | Clinical evidence / prescription | Social proof / 4.5-star rating / 10-min delivery |
| Data Owner | Hospital or clinic (fragmented, siloed) | Platform or aggregator (centralized, real-time) |
What pharma and doctors are missing is this: Every patient who chooses 10-minute relief over a clinic visit has exited the traditional healthcare system. They are not just buying a product. They are opting out of a clinical relationship.
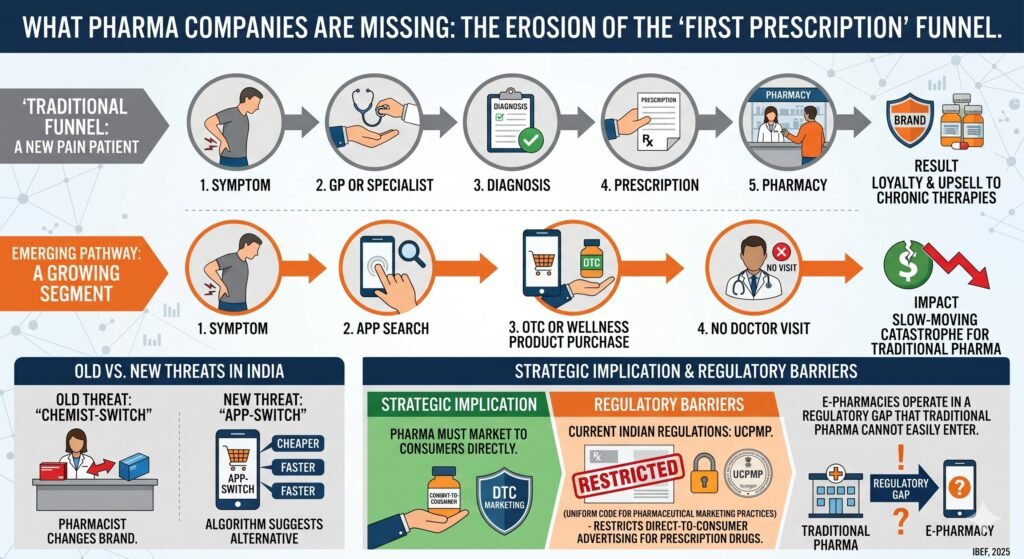
What Pharma Companies Are Missing
The Erosion of the “First Prescription” Funnel
Traditionally, a new pain patient follows a predictable path:
Symptom → GP or specialist → Diagnosis → Prescription → Pharmacy.
Now, a growing segment follows:
Symptom → App search → OTC or wellness product purchase → No doctor visit.
For pharma companies that rely on the first prescription to build brand loyalty and upsell chronic therapies, this is a slow-moving catastrophe. In India, the “chemist-switch” (where the pharmacist changes the brand) was the old threat. The “app-switch” (where the algorithm suggests a cheaper or faster alternative) is the new one.
Strategic implication: Pharma must market directly to consumers. But current Indian regulations—specifically the UCPMP (Uniform Code for Pharmaceutical Marketing Practices) —restrict direct-to-consumer advertising for prescription drugs. E-pharmacies operate in a regulatory gap that traditional pharma cannot easily enter.
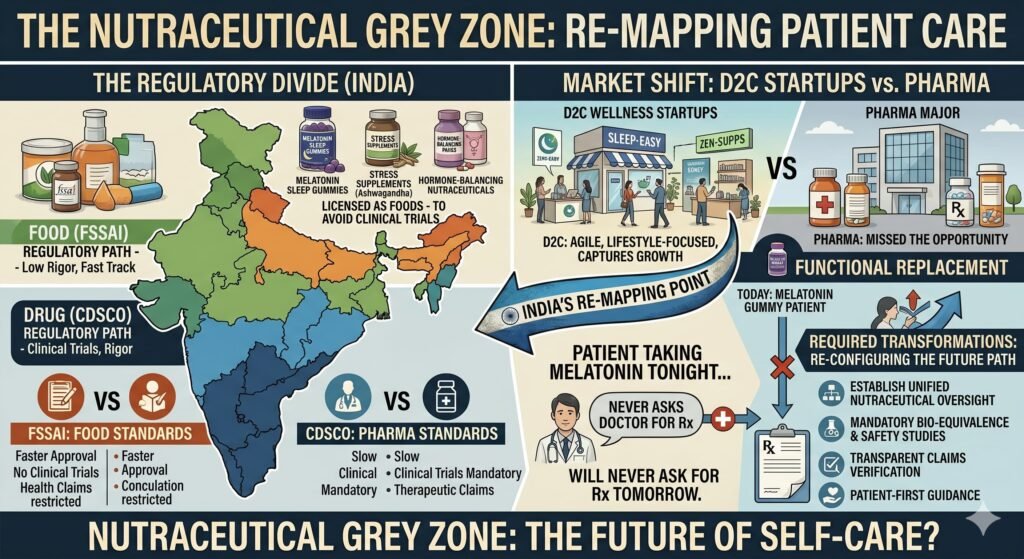
The Nutraceutical Grey Zone
The Mint article mentions sleep gummies, stress supplements, and hormone-balancing nutraceuticals. These are not classical OTC drugs. They exist in a regulatory grey zone between FSSAI and CDSCO. Many “pain gummies” and “stress supplements” are licensed as foods specifically to avoid the clinical trial rigour required for drugs.
Pharma companies have largely ignored this category, ceding it to D2C wellness startups. Meanwhile, these products are functionally replacing low-dose prescription drugs for anxiety, mild depression, and insomnia.
What pharma misses: The patient taking a melatonin gummy tonight is a patient who will never ask their doctor for a low-dose prescription tomorrow.
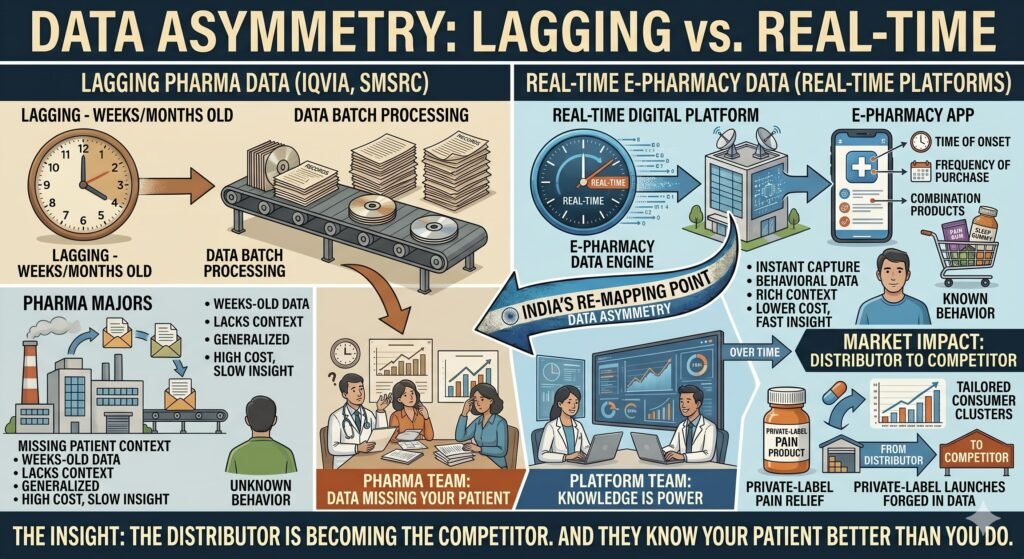
Data Asymmetry: Lagging vs. Real-Time
When a patient buys pain relief through an e-pharmacy, the platform captures real-time behavioural data: time of symptom onset, frequency of repeat purchases, and combination products (pain + sleep + digestive aids).
Pharma companies, by contrast, typically buy data from IQVIA or SMSRC—data that is lagging (weeks or months old). E-pharmacies are building richer, real-time databases of patient behaviour. Over time, this data asymmetry will allow platforms to launch their own private-label pain products, tailored to specific consumer clusters.
The insight: The distributor is becoming the competitor. And they know your patient better than you do.
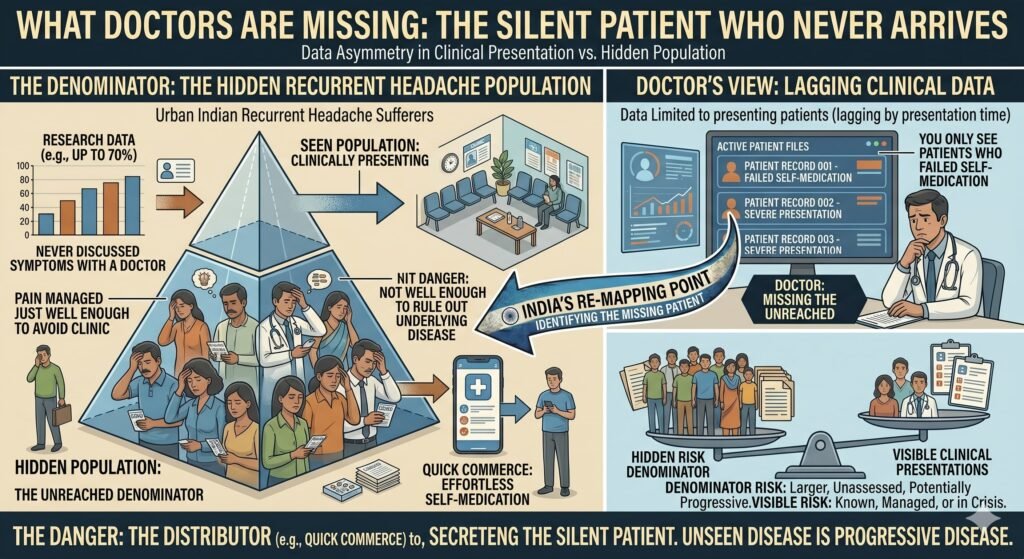
What Doctors Are Missing
The Silent Patient Who Never Arrives
The most clinically dangerous aspect of the pain economy is not the patient who self-medicates poorly. It is the patient who never presents for evaluation. Research suggests that a substantial percentage of urban Indian recurrent headache sufferers have never discussed their symptoms with a doctor. Quick commerce makes that avoidance effortless.
What doctors miss: The denominator. You only see the patients who failed self-medication. You never see the larger population whose pain is being managed just well enough to avoid a clinic visit—but not well enough to rule out serious underlying disease.
The Normalisation of Chronic Pain as a Lifestyle Feature
The Mint article astutely notes that chronic stress and fatigue are being normalised as unavoidable features of modern life. Doctors, trained to treat individual patients, are poorly equipped to counteract this cultural shift.
When a patient arrives saying, “My neck pain is just from laptop work—I use a spray, and it’s fine,” the clinical response is often a concession to patient pressure rather than a clinical intervention. It is the reality of time-strapped doctors managing patient expectations in 10-minute consultations.
What doctors miss: The opportunity to reframe pain as a diagnostic signal rather than a symptom to suppress. That requires time, trust, and continuity—all of which the instant-relief economy erodes.
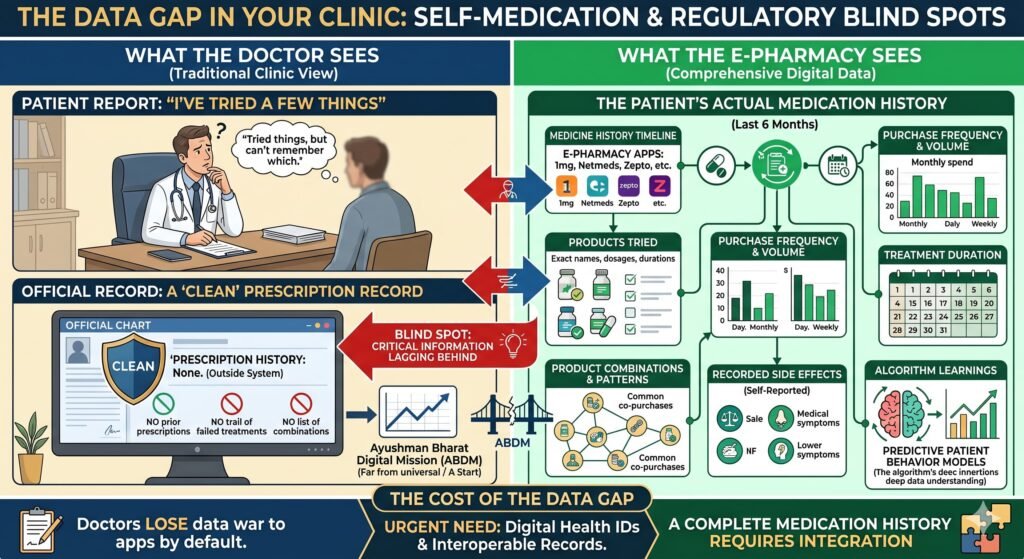
The Data Gap in Your Own Clinic
When a patient has been self-medicating with e-pharmacy products for months, what does the doctor see? A clean prescription record. No prior prescriptions. No trail of failed treatments. The patient may report “tried a few things,” but the doctor has no visibility into which products were tried, at what frequency, in what combinations, or with what side effects.
What doctors miss: A complete medication history. E-pharmacies operate outside the traditional medical record ecosystem. The Ayushman Bharat Digital Mission (ABDM) is a start, but it is far from universal. If doctors do not adopt digital health IDs and interoperable records, they will be at a disadvantage to 1mg, Netmeds, and Zepto by default.
The Platformization of Healthcare—A Power Shift
The Mint article hints at this but does not name it. In India’s under-doctored, over-stretched healthcare system, an e-pharmacy with a search bar and 10-minute delivery is, for many urban consumers, faster and more accessible than a clinic. Quality of care is not the same as speed. But for a headache at 10 PM, speed wins.
If this trend continues, e-pharmacies will evolve from fulfilment platforms to diagnostic triage systems. Some already offer chatbot symptom checkers. The logical next step is:
- AI-driven differential diagnosis
- Recommendation of OTC or prescription products
- Delivery within the hour
- Follow-up “refill reminders” that act as chronic disease management
At what point does this become the practice of medicine without a license? The National Medical Commission (NMC) is tightening regulations on unethical marketing and prescribing practices. But the regulatory arbitrage remains: tech platforms often bypass the stringent rules that traditional pharma must follow.
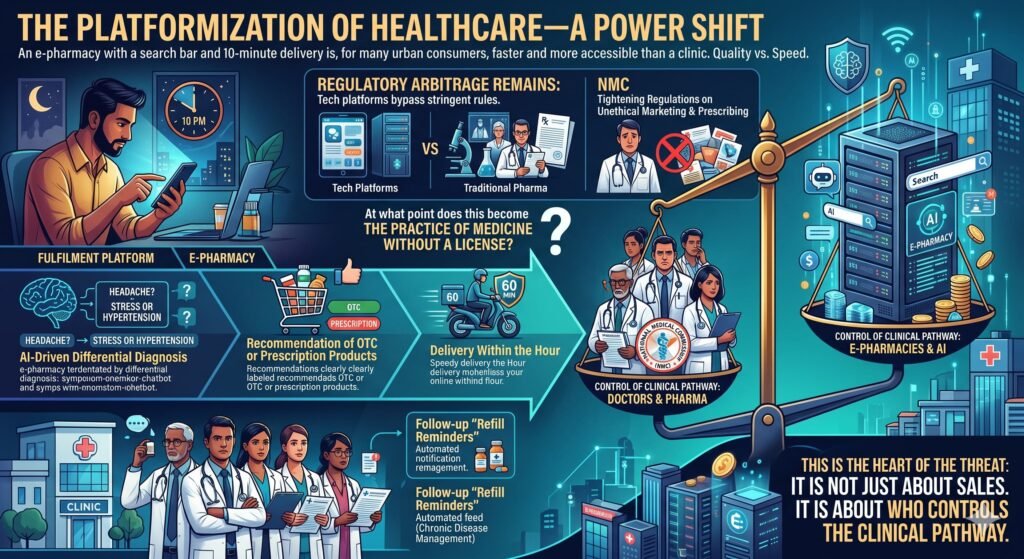
This is the heart of the platformization threat. It is not just about sales. It is about who controls the clinical pathway.
What Must Be Done Differently
For Pharma Companies: From Product-Led to Service-Led
- Stop treating e-pharmacies as just another distribution channel. They are behavioural engines. Partner with them to create clinically appropriate pathways, not just product listings.
- Invest in diagnostic tools embedded within your brand ecosystem. The company that helps a patient understand their pain before treating it wins the long game.
- Recognise that the traditional marketing playbook is obsolete. Direct-to-consumer education that drives patients toward diagnosis, not away from it, is the new imperative.
For Doctors: Reclaim the Data and the Dialogue
- Ask every pain patient: “What have you already taken from an app or pharmacy?” Document it as part of the clinical record.
- Adopt ABDM-compliant digital health IDs. Without them, you have no visibility into your patient’s real medication history.
- Educate patients explicitly on the difference between symptom suppression and diagnosis. A 30-second explanation can change a lifetime of behaviour.
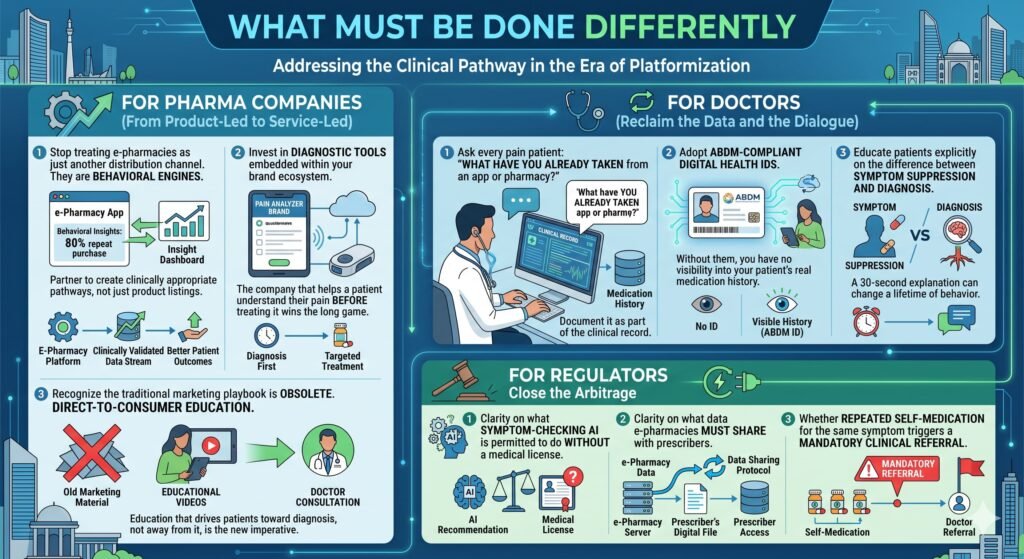
For Regulators: Close the Arbitrage
The Mint article’s public health warning is correct. India needs clarity on:
- What symptom-checking AI is permitted to do without a medical license
- What data e-pharmacies must share with prescribers
- Whether repeated self-medication for the same symptom triggers a mandatory clinical referral
The New Drugs and Clinical Trials Rules and the UCPMP provide a foundation. But they were written for a pre-platform era. They need updating.
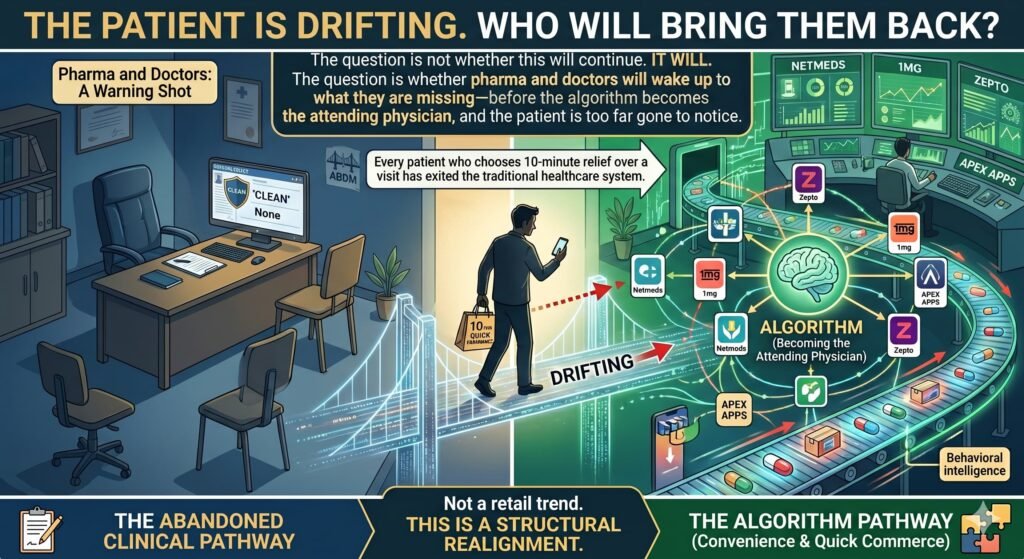
Conclusion: The Patient Is Drifting. Who Will Bring Them Back?
The Mint Lounge article is excellent journalism. But reading it as a story about convenience or consumer behaviour misses the point entirely. For pharma companies and doctors, it is a warning shot.
E-pharmacies and quick-commerce platforms are not just taking over the pain market. They are taking over the clinical pathway. Every patient who chooses 10-minute relief over a clinic visit is a patient who has exited the traditional healthcare system. That is not a retail trend. That is a structural realignment.
The question is not whether this will continue. It will. The question is whether pharma and doctors will wake up to what they are missing—before the algorithm becomes the attending physician, and the patient is too far gone to notice.
Further Reading for MedicinMan Readers
- Mint Lounge – “Quick commerce, stress and the rise of India’s pain economy”
- NMC – Latest regulations on digital health and prescribing practices
- UCPMP – Uniform Code for Pharmaceutical Marketing Practices (2023 revision)
- ABDM – Ayushman Bharat Digital Mission interoperability standards
- IQVIA / SMSRC – Market data on the shift from retail pharmacy to e-pharmacy in India





{kind=link}