
Introduction
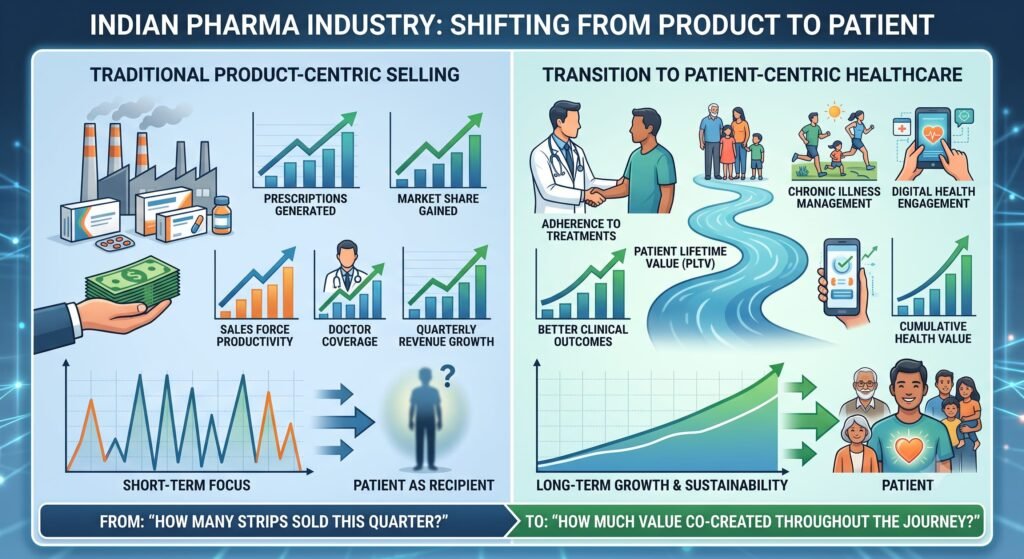
For decades, the Indian pharmaceutical industry has measured success using familiar, volume-driven metrics: prescriptions generated, market share gained, sales force productivity, doctor coverage, and quarterly revenue growth.
Yet, one critical stakeholder has remained largely absent from this commercial equation—the patient.
This omission is rapidly becoming a significant strategic vulnerability. As India’s disease burden shifts decisively toward chronic illnesses, the industry is discovering that its future depends not merely on selling more molecules, but on helping patients remain healthier, adhere to their treatments, and achieve better clinical outcomes.
The concept of Patient Life Time Value (pLTV) offers a fundamentally different way of thinking about pharmaceutical growth. Instead of asking, “How many strips of medicine did we sell this quarter?” forward-thinking leaders must ask: “How much cumulative value can we co-create with this patient throughout their entire healthcare journey?”
This distinction will define the next era of Indian pharma not a Pill-for-every-Ill paradigm.
Understanding pLTV Through Value-based Healthcare
In traditional marketing, Customer Lifetime Value refers to the total economic value gained from a customer over the course of their relationship with a brand.
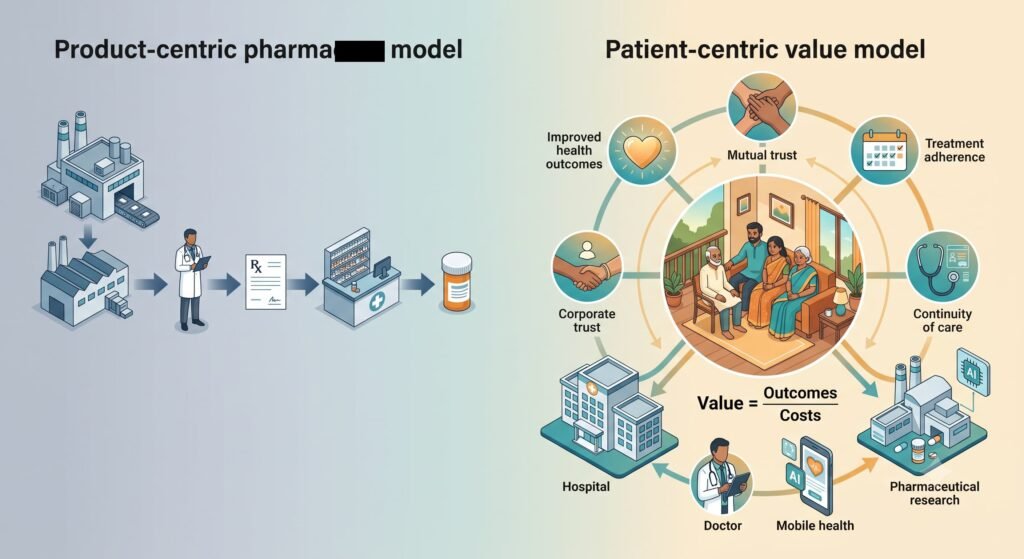
In healthcare, however, this concept requires a profound ethical and structural reinterpretation. A patient’s lifetime value is not the value extracted from their illness. Rather, it is the long-term value co-created through improved health outcomes, mutual trust, adherence, and continuity of care.
To operationalise this, we must look to the foundational formula of value-based healthcare pioneered by Michael Porter: Value equals Outcomes that matter to patients divided by Costs of delivering those outcomes
In this framework, pLTV represents the cumulative value generated over the patient’s lifetime journey. When we improve outcomes such as reducing disease progression or avoiding complications and optimise the total cost of care, the value of the entire ecosystem increases.
A patient who remains adherent to treatment, experiences fewer complications, trusts the healthcare ecosystem, receives timely disease education, and maintains regular follow-up creates sustainable value for everyone: themselves, their physicians, hospitals, and pharma companies.
The Economics Has Changed: The Indian OOP Nuance
India’s pharmaceutical market has undergone a structural transformation. Acute therapies once dominated prescriptions, but today, chronic and progressive conditions such as diabetes, hypertension, cardiovascular disease, cancer, and autoimmune disorders account for an ever-growing share of healthcare spending. Non-communicable diseases now account for approximately 60 per cent of all deaths in India, fundamentally reshaping the therapeutic landscape.
Unlike antibiotics or painkillers prescribed for a few days, chronic therapies require management that spans decades. This reality dramatically changes patient economics and introduces India’s most unique market driver: the Out-of-Pocket payer model.
Unlike in Western markets, where public or private insurance pools absorb drug costs, healthcare in India remains overwhelmingly funded out of patients’ own pockets (OOP). Current estimates indicate that approximately 60-70% of healthcare spending in India is out-of-pocket. In an OOP ecosystem, the patient is simultaneously the consumer, the payer, and the primary decision-maker.
This dual role changes how pLTV must be calculated and managed.
The Affordability-Adherence Loop: When a patient must pay for their daily medication out of their monthly household budget, financial toxicity is the leading cause of therapy abandonment. Studies on chronic disease management in India have consistently found cost to be the primary barrier to sustained treatment adherence.
The Value Perception: If a patient does not perceive tangible, ongoing improvement in their quality of life, they will stop buying the drug. Every missed refill, discontinued medication, or preventable complication represents lost value—both to patient health and to long-term Pill-for-every-Ill sustainability.
In India, pLTV cannot be managed solely through clinical efficacy. It must be managed through an integrated approach to affordability, accessibility, and continuous value demonstration.

The Evolving Payer Ecosystem
While the out-of-pocket model remains dominant, India’s healthcare financing landscape is evolving. Three significant developments are reshaping the payer mix and, consequently, how pLTV must be understood.
First, government-sponsored insurance schemes such as the Pradhan Mantri Jan Arogya Yojana, or PMJAY, have expanded coverage to millions of economically vulnerable families. PMJAY alone provides health insurance coverage of up to five lakh rupees per family per year for secondary and tertiary care hospitalization. This shifts the economic burden away from patients and creates different adherence dynamics, though implementation challenges and hospital coverage limitations remain.
Second, private health insurance penetration is growing, particularly among urban, middle-class populations. As more patients become insured, the direct financial friction that drives therapy abandonment may reduce, but new complexities emerge around insurance reimbursement processes, formulary restrictions, and co-payment requirements.
Third, corporate health insurance through employers now covers a significant portion of the formal workforce. This creates opportunities for workplace wellness programs and chronic disease management initiatives that can improve adherence.
For pharmaceutical companies, these developments mean that pLTV strategies must be nuanced across different payer segments. An uninsured patient in rural India requires a fundamentally different support model than an insured corporate employee in a metropolitan city. The affordability-adherence loop operates differently, and the value proposition must adapt accordingly.

India’s Biggest Challenge Is Not Access—It Is Adherence
The industry’s greatest opportunity is no longer simply launching the next molecular entity. It is helping existing patients successfully continue the therapies they have already been prescribed.
The World Health Organization has long documented that only about half of patients with chronic diseases take their long-term medications as prescribed. This finding has been replicated across multiple international studies. In India’s self-funded market, the situation is often more pronounced.
Studies examining adherence to chronic therapies in India paint a concerning picture. Research on diabetes management has found adherence rates ranging from 40 to 60 per cent in various settings. Hypertension studies show similar patterns, with a significant proportion of patients discontinuing therapy within the first year. A study published in the Indian Journal of Medical Research found that only 42 per cent of diabetic patients were adherent to their oral hypoglycemic agents.
The reasons are multifaceted. Financial constraints are paramount, but other barriers include inadequate patient education about the disease and its progression, fragmented care across multiple providers without proper coordination, lack of structured follow-up mechanisms, and limited understanding of the importance of long-term therapy, especially when symptoms are not immediately apparent.
A patient who abandons therapy benefits no one. Not the physician who designed the treatment plan. Not the pharmaceutical company that manufactured the medicine. And most importantly, not the patient whose health is compromised.
Why Product-centric Pharma Is Reaching Its Limits
Historically, Indian pharma perfected the doctor-centric commercial model. The value chain was straightforward: Manufacture, then promote to the doctor, then prescription, then pharmacy sale.
This transactional model worked exceptionally well in an era dominated by acute care and basic branded generics. But managing chronic care requires a completely different operating model. Success is no longer determined at the point of sale. It is determined by what happens after the prescription is written.
Does the patient understand their chronic condition?
Can they sustain the monthly cost of treatment?
Are they taking the medication correctly and managing side effects?
Are their clinical markers actually improving over time?
These post-prescription variables are the true determinants of real-world therapeutic effectiveness. The pharma company that ignores these questions is, in effect, abandoning its patients after the point of sale.
Consider the contrast. A product-centric company measures success by market share and prescription volume. It invests heavily in physician engagement and sales force deployment. Its commercial success is measured quarterly and transactionally. A patient-centric company, by contrast, measures success by treatment persistence, patient satisfaction, clinical outcomes, and health-related quality of life. It invests in patient education, adherence support, and digital health tools. Its commercial success is measured longitudinally and relationally.
The limitations of the product-centric model become starkly apparent in chronic disease management. When the goal is simply to sell more tablets, the company has no incentive to ensure that those tablets are actually being taken correctly. When the goal is patient health, the company has every incentive to ensure therapy success.
The Rise Of Patient-centric Pharma: Managing Journeys, Not Pills
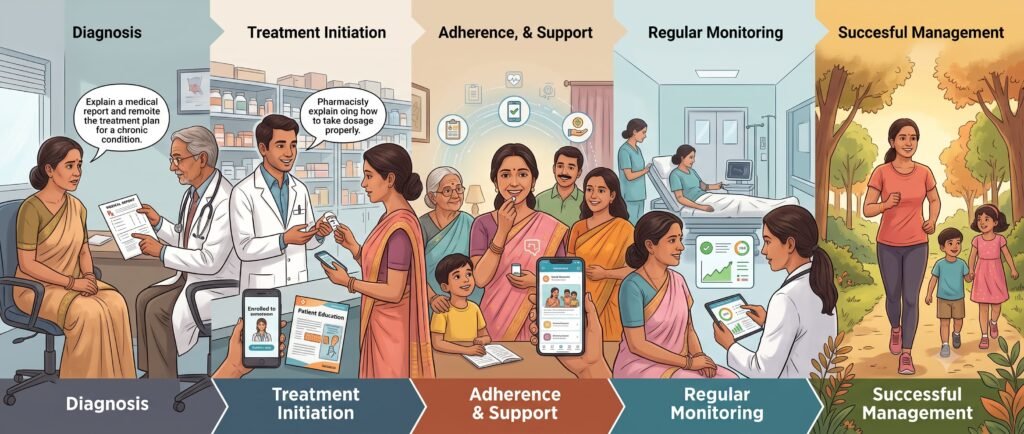
Globally and locally, progressive pharmaceutical companies are expanding their scope beyond the pill. They are beginning to offer integrated ecosystems that include personalized disease education and digital support groups, direct-to-patient adherence programs and financial assistance, remote monitoring, lifestyle coaching, and nutrition guidance, as well as continuous tracking of Patient-Reported Outcomes to measure real-world quality of life.
These initiatives are not corporate social responsibility. They are core business strategies. They improve treatment persistence, foster brand trust, and secure long-term commercial viability in a highly competitive market.
Consider diabetes. The medicine itself represents only a fraction of successful clinical management. Long-term health depends on nutrition, regular glucose monitoring, physical activity, renal screenings, and cardiovascular risk reduction. The pharma company that helps integrate these elements creates substantially greater pLTV than one that sells tablets.
One leading Indian pharmaceutical company implemented a comprehensive patient support program for its diabetes portfolio, including personalized counseling, digital reminders, and financial assistance for eligible patients. Within eighteen months, the program demonstrated a measurable improvement in medication adherence and a reduction in therapy abandonment rates. Patients enrolled in the program showed significantly better glycemic control compared to those receiving standard care.
Another example involves a multinational company operating in India that developed a mobile application for cancer patients. The app provided education on treatment, side-effect management, and appointment reminders, and served as a platform for patients to report symptoms directly to their care team. The result was improved treatment persistence and enhanced patient satisfaction scores.
These examples illustrate the fundamental shift. The pharma company is no longer merely a Pill-for-every-Ill peddler. It must become an active partner in the health management journey.
The AI Opportunity
Artificial Intelligence is the catalyst that can finally make individualized pLTV scalable. Rather than treating patients as uniform demographic blocks, AI allows pharma to personalize the care journey at scale.
Predictive Adherence Models represent the first major application. By analyzing behavioral patterns, prescription refill histories, demographic data, and social determinants of health, AI algorithms can identify which patients are at high risk of dropping off therapy. This enables early intervention before therapy abandonment occurs. A study published in the Journal of Medical Internet Research demonstrated that machine learning models could predict medication non-adherence with significant accuracy, allowing healthcare providers to target support to those most in need.
Dynamic Digital Coaching is the second frontier. AI-powered systems can deliver personalised, real-time reminders and lifestyle tips tailored to an individual’s daily routine. These systems can adapt to patient preferences, learning what types of communication work best for each individual. They can provide motivational messaging, educational content, and behavioural nudges at the right time and through the right channel.
Optimized Adverse-Event Management is the third area of opportunity. AI can help patients identify and manage mild side effects before they lead to therapy discontinuation. By analyzing patient-reported symptoms and comparing them to known patterns, AI systems can provide early warnings and guidance. This proactive approach can prevent the side effect spiral that often leads to treatment abandonment.
Indian companies are particularly well-positioned to leverage AI given the country’s world-class software development capabilities. Several Indian pharmaceutical companies have already begun developing proprietary AI platforms for patient engagement, though widespread adoption remains in its early stages.
India’s Competitive Advantage
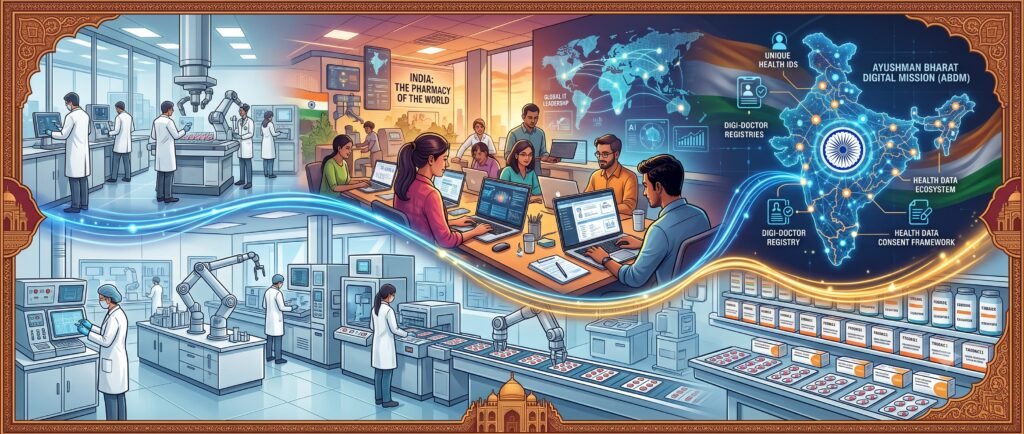
India is uniquely positioned to pioneer this transition. The nation possesses a powerful triad of capabilities.
First, there is a world-class pharmaceutical manufacturing base. India is the pharmacy of the world, with a robust generic drug industry and growing capabilities in biosimilars and complex formulations. This manufacturing excellence ensures that high-quality medicines are available at accessible prices.
Second, there is unrivaled global IT and software development expertise. India has built a formidable technology industry, with deep capabilities in artificial intelligence, data analytics, and digital platform development. This talent pool can be mobilized to create the digital health tools that patient-centric care requires.
Third, there is a rapidly evolving public digital health infrastructure, anchored by the Ayushman Bharat Digital Mission. Launched in 2021, ABDM aims to create a national digital health ecosystem including unique health IDs, digi-doctor registries, and health data consent frameworks. As this infrastructure matures, it will enable seamless data sharing and coordinated care across the healthcare system.
The next major competitive advantage for Indian pharma will not come from low-cost generic manufacturing alone. It will come from the ability to synthesize medicines with digital health platforms, localized diagnostics, and continuous patient-support services.
Indian pharmaceutical companies that build this synthesis capability will not only dominate the domestic market but will also export this model to other emerging economies facing similar healthcare challenges. The patient-centric care model developed for India could become a global template for pharmaceutical engagement in resource-constrained LMIC settings.

The Ethical Dimension of pLTV
There is an understandable risk that applying the term lifetime value to a patient could be misinterpreted as a desire to maximize revenue from lifelong illness. That view is fundamentally incorrect.
The purpose of patient-centric healthcare is not to maximise the duration of treatment, but to maximise the duration of health.
This distinction matters profoundly. There is an inherent tension in pharmaceutical business models. The moral imperative must intentionally counterbalance the economic incentive to extend treatment to restore health. Companies that structure their strategies around outcome-based models, rather than volume-based ones, will ultimately be more sustainable and more trusted.
The highest form of value creation in medicine remains preventing disease progression, managing conditions to avoid acute crises, or curing them outright. Innovations like precision medicine, targeted biologics, and preventive vaccines demonstrate that true value lies in restoring health, not maintaining chronic dependence.
Consider the pharma company that develops a curative therapy for a chronic condition. Its revenue from that particular therapy may decline, but its reputation, trust, and long-term relationship with patients and physicians will be enhanced. The company becomes known as a genuine health partner, not merely a Pill-for-every-Ill supplier.
Our success as an industry must ultimately be measured by the healthy years we return to patients, not by the number of prescriptions renewed indefinitely. This is not naivety. It is the recognition that in the long run, what is good for patients is good for business. Trust, once earned, creates durable competitive advantage.
This perspective also requires honest acknowledgment that the transition from volume-based to value-based models requires structural changes in how pharma companies are organised, incentivised, and measured. Short-term revenue pressures must be balanced against long-term relationship building. Sales force incentives must evolve to reward patient outcomes, not just prescription volume. These changes are difficult but essential.
Conclusion
Indian pharma has mastered manufacturing. We have mastered branded generics. We have mastered physician engagement. Our next frontier is deep, meaningful patient engagement. The companies that will lead the next decade will not necessarily be those with the largest sales forces or the most crowded portfolios. They will be those that understand an enduring truth.
Pill-for-every-Ill creates transactions. Better health creates relationships.
The lifetime value of a patient is not measured in prescriptions filled. It is measured in healthier, high-quality years lived.
The question for Indian pharma leaders is not whether to adopt patient-centric approaches. It is how quickly they can build the capabilities to do so. The journey begins with one question: How well do you truly know your patients?
The transition from product-centric selling to patient-centric healthcare is not merely a strategic choice. It is an imperative driven by the changing disease burden, the economic realities of the Indian market, the possibilities created by digital technology, and the moral responsibility of healthcare companies to those they serve.
Indian pharma has always been resilient, adaptive, and entrepreneurial. The patient-centric transformation offers an opportunity to apply those qualities to the most important stakeholder in the healthcare ecosystem. It is time to move beyond Pill-for-every-Ill and embrace the person.

APPENDIX: REFERENCES
- Porter, M. E. (2010). What Is Value in Health Care? New England Journal of Medicine, 363(26), 2477-2481. This article establishes the foundational formula of healthcare value as outcomes achieved per dollar spent and provides the conceptual framework for value-based healthcare delivery.
- World Health Organization. (2003). Adherence to Long-Term Therapies: Evidence for Action. Geneva: WHO Press. This comprehensive report documents the global challenge of medication adherence, establishing that only about half of patients with chronic diseases take their medications as prescribed, and provides evidence-based recommendations for improving adherence.
- Brown, M. T., & Bussell, J. K. (2011). Medication Adherence: WHO Cares? Mayo Clinic Proceedings, 86(4), 304-314. This article updates and expands upon the WHO adherence findings, exploring the multiple dimensions of adherence and the interventions that can improve it.
- Kumar, R., & Narula, D. (2020). Medication Adherence in Chronic Diseases: An Indian Perspective. Indian Journal of Community Medicine, 45(3), 267-272. This study examines adherence patterns in chronic disease management in India, identifying cost, access, and patient education as key barriers to sustained therapy.
- Patel, V., Chatterjee, S., & Chisholm, D. (2017). Chronic Diseases and Healthcare in India: The Challenge of Adherence. Indian Journal of Medical Research, 145(4), 435-441. This research documents adherence rates for various chronic conditions in Indian settings and explores the socioeconomic factors influencing treatment persistence.
- Gupta, R., & Mohan, V. (2019). Out-of-Pocket Expenditure and Catastrophic Health Spending in India: Implications for Chronic Disease Care. Journal of Health Economics, 68, 102240. This economic analysis quantifies the out-of-pocket burden of chronic disease management in India and its impact on treatment adherence.
- OECD. (2017). Caring for Quality in Health: Lessons Learnt from OECD Reviews of Health Care Quality. OECD Publishing. This publication highlights how patient-centered care directly correlates with improved therapeutic adherence and system efficiency across multiple healthcare systems.
- OECD. (2020). Realising the Potential of Primary Health Care. OECD Publishing. This report analyzes international frameworks for people-centered healthcare and examines the critical role of self-management in chronic disease management.
- Rotenstein, L. S., Huckman, R. S., & Wagle, N. W. (2017). Making Patients and Doctors Happier—The Potential of Patient-Reported Outcomes. New England Journal of Medicine, 377(14), 1309-1312. This article demonstrates how tracking outcomes reported directly by patients improves overall care quality and enhances the patient-provider relationship.
- Patient-Centered Outcomes Research Institute. (2022). Patient-Centered Value in Health and Health Care. PCORI Policy Brief. This policy document outlines the integration of patient goals, equity, and transparency into clinical value models and provides guidance for outcome measurement.
- van den Berg, M. J., et al. (2023). Does Value-Based Healthcare Support Patient-Centred Care? A Systematic Review. BMJ Open, 13(5). This systematic review evaluates the gap between provider-focused metrics and genuine patient-centered outcomes in modern medicine.
- NITI Aayog. (2021). Digital Health India: Progress and Potential. Government of India Publication. This report provides an overview of the Ayushman Bharat Digital Mission and assesses the current state and future potential of digital health infrastructure in India.
- National Health Authority. (2022). Ayushman Bharat Pradhan Mantri Jan Arogya Yojana: Annual Report. Government of India. This document outlines the coverage, implementation, and impact of India’s largest government-sponsored health insurance scheme.
- Sim, J. Y., & Kim, J. (2020). Machine Learning for Predicting Medication Adherence: A Systematic Review. Journal of Medical Internet Research, 22(7), e18678. This systematic review demonstrates the capability of machine learning models to predict medication non-adherence with significant accuracy, enabling targeted intervention.
- Iyengar, V., & Sharma, A. (2021). Digital Therapeutics and Patient Engagement in India: Emerging Models. Indian Journal of Pharmacology, 53(5), 389-395. This article examines the growing role of digital tools in patient engagement and chronic disease management in the Indian context.
- International Diabetes Federation. (2022). IDF Diabetes Atlas, 10th Edition. Brussels: IDF. This atlas provides global and regional data on diabetes prevalence, management, and complications, including specific data for India.
- World Health Organization. (2018). Noncommunicable Diseases Country Profiles: India. Geneva: WHO Press. This country profile documents the burden of non-communicable diseases in India and provides baseline data for health policy planning.
- Tripathi, S., & Singh, R. (2020). Patient Support Programs in the Indian Pharmaceutical Industry: Current Status and Future Directions. Pharma Times, 52(8), 12-18. This industry analysis examines the adoption and effectiveness of patient support programs among Indian pharmaceutical companies.
- Reddy, K. S., & Gupta, M. (2019). Healthcare Financing in India: From Out-of-Pocket to Universal Health Coverage. Economic and Political Weekly, 54(28), 45-52. This article traces the evolution of healthcare financing in India and discusses the transition toward universal health coverage.
- The Lancet Global Health. (2020). Digital Health in India: Challenges and Opportunities. The Lancet Global Health, 8(9), e1108-e1110. This commentary provides a balanced assessment of digital health opportunities in India while acknowledging implementation challenges and equity concerns.




{kind=link}