
When a vial contains only water, the failure is not merely pharmaceutical—it is institutional.
On paper, India is the Pharmacy of the World. It supplies around one in every five generic medicines consumed globally, manufactures more than 60,000 pharmaceutical products, and exports medicines to over 200 countries. It has earned global respect for affordable vaccines, complex generics, and increasingly sophisticated biologics.
Yet every few years, another tragedy reminds us that India’s pharmaceutical ecosystem has a dangerous dual personality.
One India manufactures world-class medicines under the most stringent international regulatory oversight.
The other manufacturers of drugs in obscure facilities that few have heard of—until patients die.
The investigation into Punjab-based Jackson Laboratories Pvt. Ltd., following the deaths of five young mothers in Rajasthan, is not simply a story about one allegedly defective batch of oxytocin. It is a case study in how regulatory blind spots, fragmented oversight, weak procurement systems, and poor accountability allow questionable manufacturers to survive—and sometimes thrive—within India’s healthcare ecosystem.
A Tragedy That Should Never Have Happened
Between May 5 and May 17, 2026, five women who underwent Caesarean deliveries at the Government Medical College Hospital in Kota died after developing a strikingly similar clinical picture: sudden hypotension, kidney failure, severe bleeding, dialysis, and ultimately death .
All had received oxytocin injections after childbirth.
Laboratory testing by Rajasthan authorities reportedly found that the suspect batch of oxytocin—marketed as Tocin, Batch I-7881, manufactured by Jackson Laboratories—contained no detectable oxytocin. According to investigators, the vials effectively contained water rather than the labelled active pharmaceutical ingredient .
Jackson Laboratories has contested this finding and moved a Kota court seeking retesting of the batch. Rajasthan has sent samples to a drug-testing laboratory in Kolkata, and officials have said proposed prosecution will remain on hold until the fresh report is received .
The scientific questions remain open.
The governance questions do not.

Jackson Laboratories Was Not an Unknown Company
Contrary to public perception, Jackson Laboratories was not an unlicensed backyard operation.
It was a registered pharmaceutical manufacturer supplying government institutions across India. Its portfolio extended far beyond oxytocin to cardiovascular drugs, diabetes medicines, antibiotics, thyroid products, nutritional supplements and injectables.
This was not a company operating outside the system.
It was operating squarely inside it.
That is precisely what makes the case disturbing.

The Regulatory History Nobody Connected
Perhaps the most uncomfortable question is whether warning signs existed long before the Kota tragedy.
A joint inspection by the Central Drugs Standard Control Organisation (CDSCO) and the Punjab drug regulator, conducted under the risk-based inspection framework, identified 58 critical observations and 451 major observations at Jackson Laboratories’ Punjab facility .
According to investigation documents accessed by The Economic Times, the team found that the firm had not performed any testing for the impugned product or finished product. “The team opined that the certificate of analysis submitted by the firm is not reliable,” an official said.
Investigators also reported that, instead of using water from a reverse osmosis (RO) plant, tap water was processed directly at the manufacturing site.
“The firm is not following principles of GMP (good manufacturing practices) at any stage,” the report said, adding that products were found stored under unhygienic conditions.
The manufacturing area was dirty, and the tablet section opened directly to the outside. The critical area of the parental department lacked controlled area status. Multiple tablet punching machines were kept in a common area. Batches were manufactured with no identification, no batch records and no documentation. Reject bottles, loose labels and printed blister rolls lay scattered across production areas .
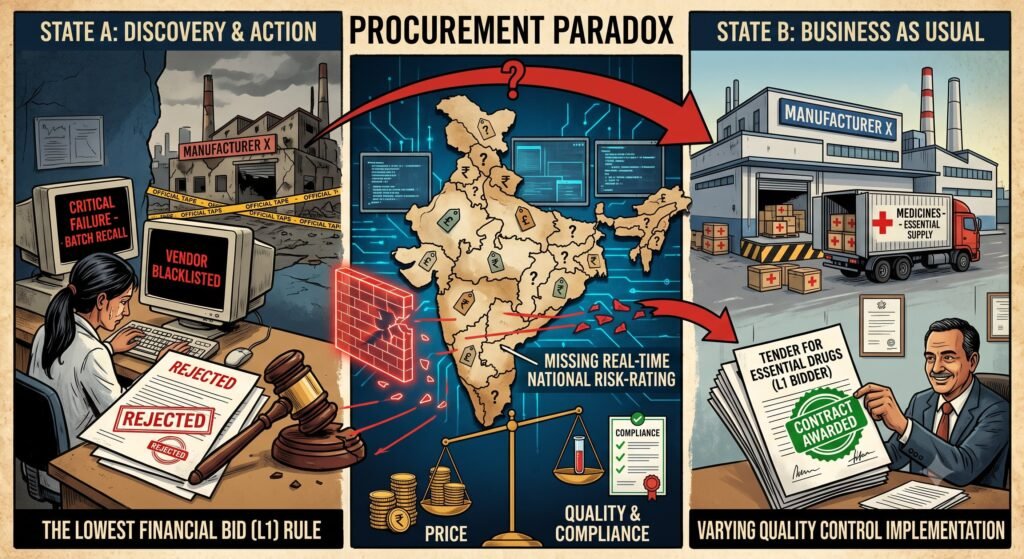
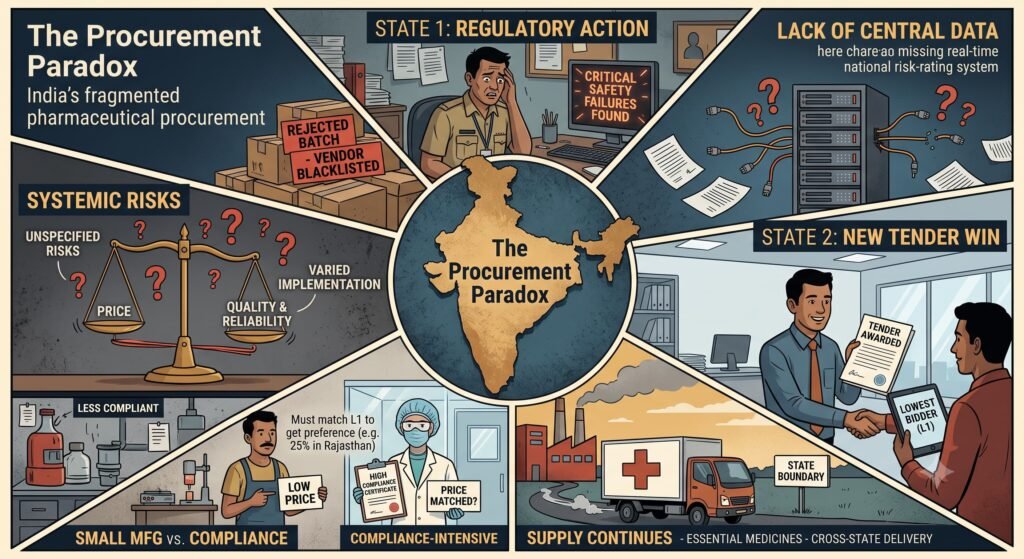
The Procurement Paradox
One of the most surprising revelations is that manufacturers facing regulatory action in one state may continue supplying medicines to hospitals in another.
India has no universally implemented, real-time national supplier risk-rating system that automatically flags manufacturers with repeated quality failures to all procurement agencies.
Consequently, a company may:
- lose a contract in one state,
- continue winning tenders elsewhere,
- continue supplying essential medicines,
- continue expanding business.
This is not necessarily illegal.
But it is undeniably risky.
Government procurement often prioritises the lowest financial bid (L1) . Under Rajasthan’s procurement policy, purchase preference is restricted to 25% (10% for state PSUs and 15% for state SSIs), and only on condition that they match the L1 rates obtained through tendering .
While quality control mechanisms exist on paper—including random sampling, third-party laboratory testing, and blacklisting provisions for substandard drugs—implementation varies across jurisdictions .
Smaller manufacturers, able to undercut larger, compliance-intensive companies, can remain competitive unless procurement systems effectively account for past compliance performance.
The result is a procurement ecosystem where price can overshadow quality.
India’s Two Pharmaceutical Industries
The Jackson episode should not become an indictment of the entire Indian pharmaceutical industry.
That would be inaccurate and unfair.
India today hosts many globally respected manufacturers inspected regularly by regulators including the US FDA, EMA, MHRA, PMDA and TGA. These companies invest heavily in quality systems, validation, data integrity, pharmacovigilance and regulatory compliance.
The concern lies elsewhere.
India also has hundreds of small and mid-sized manufacturers that primarily serve domestic government procurement or low-margin institutional markets. Many operate with far fewer external inspections than export-oriented companies.
The quality gap between these two segments can be substantial.
International regulators often inspect export plants more rigorously than facilities producing solely for the domestic market.
Ironically, Indian patients may sometimes receive medicines manufactured under less stringent oversight than those exported overseas.

The Cost of Fragmented Regulation
India’s pharmaceutical regulation remains divided between central and state authorities.
At the central level, the CDSCO, headed by the Drug Controller General of India, regulates licensing, approvals, oversight, marketing, manufacture, quality control and distribution of drugs under the Drugs and Cosmetics Act, 1940 . At the state level, State Drug Controllers operate under the CDSCO’s overall supervision, regulating licensing, manufacturing, marketing and distribution within their jurisdictions .
This decentralised structure can create uneven enforcement, inconsistent inspection quality, delayed information sharing and varying procurement standards.
When a drug loses its “new drug” status after four years, the authority to grant manufacturing permissions shifts from the Central Licensing Authority to State Licensing Authorities. This creates potential regulatory gaps, particularly for patent and proprietary medicines where specifications and analytical procedures are not in the public domain .
The Jackson case illustrates why these structural issues matter.
A medicine manufactured in Punjab may be procured in Rajasthan, distributed through another agency, investigated by a third authority and scrutinised internationally only after patients die.
No single regulator necessarily has a complete picture.

The Global Dimension
The World Health Organisation has sought additional information from the Government of India regarding the oxytocin injections and the deaths in Kota.
Ministry sources clarified that the WHO’s communication is a routine part of the global pharmacovigilance and regulatory surveillance mechanism. The organisation regularly seeks information from national regulatory authorities to determine whether such incidents are confined to a particular location or whether there could be implications for other countries where the product may have been distributed .
Officials stressed that the WHO’s request should not be construed as a finding against the product or the manufacturer, but as part of the standard international process of assessing potential public health risks.
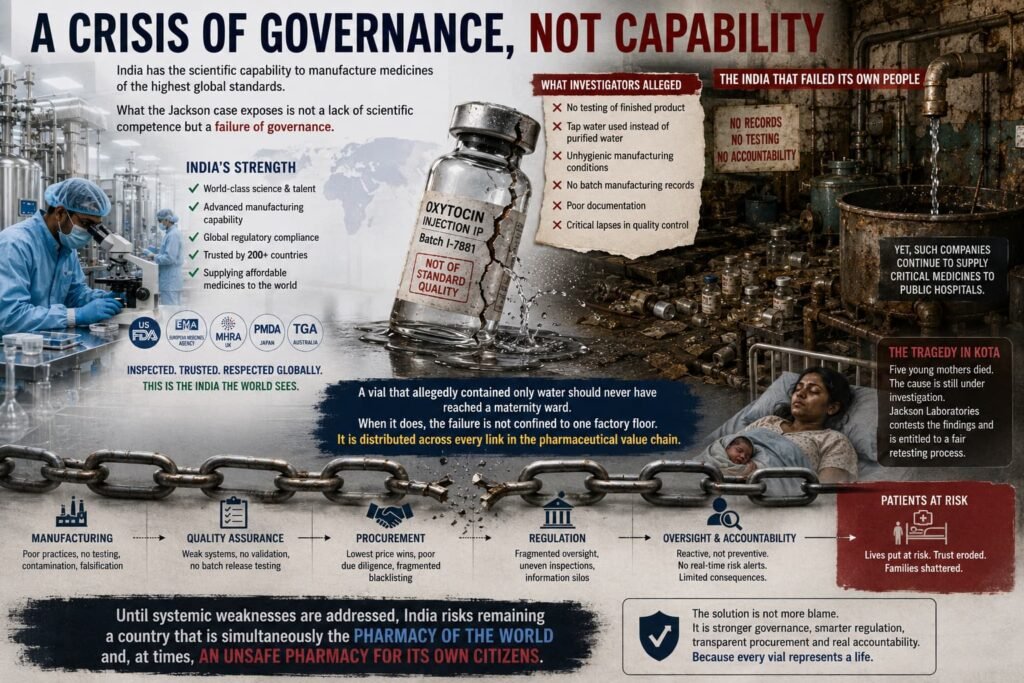
A Crisis of Governance, Not Capability
India unquestionably possesses the scientific capability to manufacture medicines of the highest global standards.
What the Jackson case exposes is not a lack of scientific competence but a failure of governance.
When a company that allegedly failed to perform any testing on its finished product, used tap water instead of purified water in manufacturing, and operated in unhygienic conditions without batch records, continues supplying critical medicines to public hospitals, the issue extends beyond one manufacturer.
It reflects a system where information remains fragmented, accountability is reactive rather than preventive, and procurement struggles to distinguish between consistently compliant manufacturers and those with recurring quality concerns.
The tragedy in Kota is still under investigation, and the cause has not been finally established. Jackson Laboratories has contested the findings and is entitled to a fair retesting process.
But one conclusion is already difficult to escape.
A vial that allegedly contained only water should never have reached a maternity ward.
When it does, the failure is not confined to one factory floor.
It is distributed across every link in the pharmaceutical value chain—from manufacturing and quality assurance to procurement, regulation and oversight.
Until those systemic weaknesses are addressed, India risks remaining a country that is simultaneously the Pharmacy of the World and, at times, an unsafe pharmacy for its own citizens.
Appendix: Verified Source References
| Source | Key Information Provided |
|---|---|
| The Times of India (June 27, 2026) | Jackson Laboratories contests “spurious” finding; court-ordered retesting in Kolkata; distributor licence cancelled |
| Outlook India (June 26, 2026) | WHO seeks details; Centre cancels licences after GMP inspection findings |
| Rajasthan Medical Services Corporation | Official drug procurement policy documentation; L1 bidding system; quality control mechanisms |
| The Hindu (June 26, 2026) | WHO seeks information; manufacturing licences cancelled following joint CDSCO inspections |
| ET Pharma (June 27, 2026) | 58 critical observations and 451 major observations at Jackson’s Punjab facility; no testing performed; tap water used instead of RO water; unhygienic conditions |
| azb Partners (January 2026) | Overview of India’s two-tiered pharmaceutical regulatory framework (CDSCO + State Drug Controllers) |
| Express Pharma (November 2025) | Analysis of regulatory gaps when new drug status lapses; transfer of authority from central to state licensing authorities |
| The New Indian Express (June 26, 2026) | Centre cracks down on Jackson Laboratories; WHO seeks information |
| ETV Bharat (June 27, 2026) | WHO communication routine pharmacovigilance; government awaiting Rajasthan report |




{kind=link}