
The Data Graveyard: Why India’s Private Hospitals Fail at Medical Research
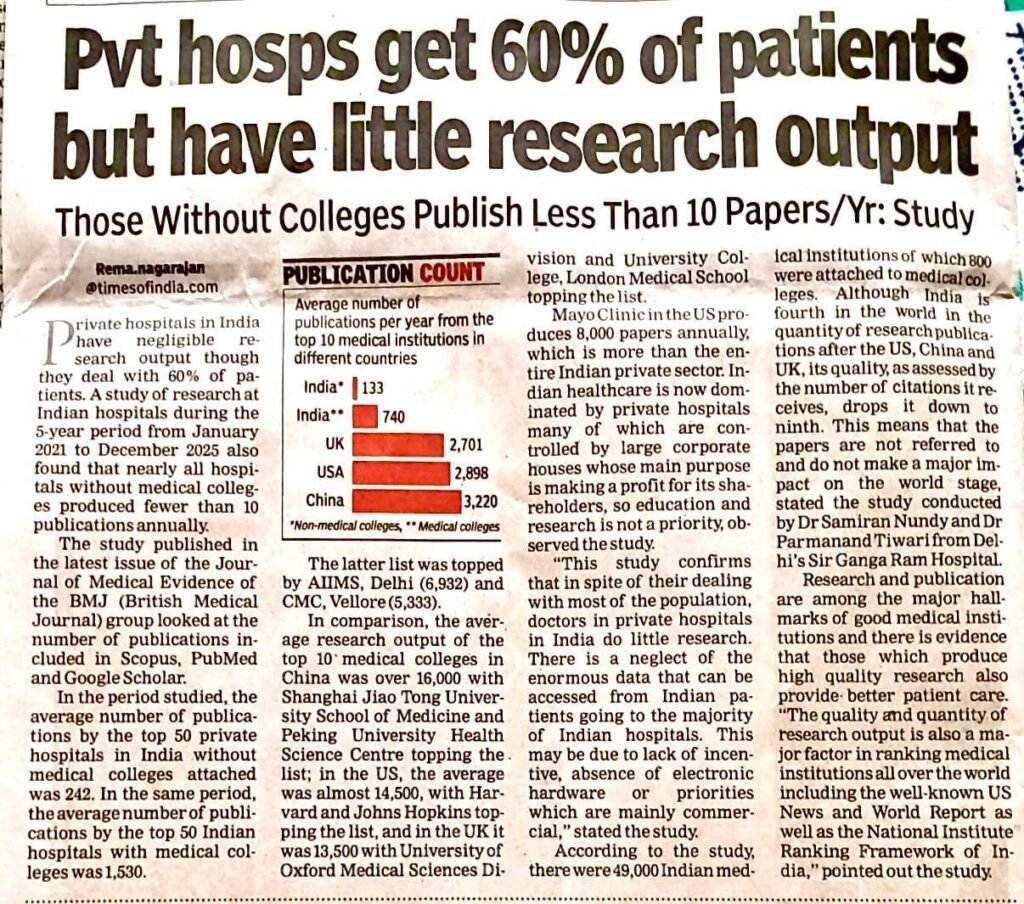
In India, the medical landscape presents a glaring paradox: private hospitals treat roughly 60% of the nation’s patients, yet the vast majority of institutions without attached colleges produce fewer than 10 research papers a year on average. Meanwhile, public medical colleges and premier academic centres carry almost the entire burden of the nation’s medical research output. A recent study published in the Journal of Medical Evidence (BMJ Group) has exposed this systemic failure. Conducted by Dr Samiran Nundy and Dr Paramanand Tiwari from Delhi’s Sir Ganga Ram Hospital, the study analysed research output from January 2021 to December 2025 across Scopus, PubMed, and Google Scholar. Their findings reveal a troubling reality: while India ranks 4th globally in the sheer volume of medical publications, it drops to 9th in citation impact. The country treats millions, but it is failing to learn from them. Here is a deep dive into what India is missing, why it matters, and how to fix it.
1. The Missing “Clinical” Insight
India has a massive, diverse, and genetically unique population. Private hospitals possess terabytes of Electronic Health Records (EHR) data on rare tropical diseases, cardiovascular anomalies, and unique drug responses.
What India is missing:
The translation of this data into localized clinical guidelines. While the Mayo Clinic in the US alone produces 8,000 papers annually utilizing its patient data—surpassing the output of India’s entire private hospital sector—India’s private sector allows its data to sit dormant. This neglect means global medical protocols remain largely written based on Western populations, which often do not respond identically to Indian patients (such as differing genetic responses to statins or anticoagulants).
2. The Missing “Knowledge Economy”
The study highlights a fundamental structural flaw: corporate priorities versus academic missions. In India, most prominent private hospital chains are controlled by large corporate houses. Their primary fiduciary duty is to shareholders, meaning education and research are rarely prioritized.
What India is missing:
Time, incentives, and infrastructure. In a commercial private setup, a clinician’s value is heavily measured by “patient turnover” and billable procedures. Research requires sabbaticals, dedicated statisticians, and long-term patient follow-ups—none of which align with immediate profit margins. The culture of robust academic publishing primarily exists in dedicated medical colleges, such as the government-run AIIMS Delhi or premier private institutions like CMC Vellore. However, hospitals operating purely as commercial centers remain research deserts.
3. The Missing “Global Impact”
As noted by the study’s authors, Indian papers are frequently ignored on the world stage. The US, UK, and China dominate high-impact medical journals because their research asks fundamental, global questions. Top medical colleges in China average over 16,000 publications, while the top 10 in the US average nearly 14,500.
What India is missing:
Citations. Because much of the research coming out of non-collegiate Indian hospitals lacks scale or rigorous infrastructure, it is rarely referred to by international peers. Without high citation counts, Indian discoveries do not influence global surgical guidelines, oncology protocols, or emergency medicine standards. India remains a “consumer” of global medical knowledge rather than a “creator.”
4. The Missing Interface: Academia and Industry
The study notes that of the approximately 49,000 medical institutions in India, only a tiny fraction—800—are attached to medical colleges and actively contributing to the research ecosystem.
What India is missing:
A collaborative bridge. In developed nations, private healthcare networks routinely partner with university research wings. The private hospital provides the patient volume and clinical data; the university provides the intellectual rigor, biostatisticians, and lab infrastructure. In India, these two worlds remain entirely siloed due to regulatory hurdles, a lack of standardized data-sharing protocols, and a deficit of commercial incentives.
The Path Forward: How to Bridge the Gap
India desperately needs localized research to lower healthcare costs, improve drug efficacy, and develop home-grown medical devices. To turn this around, systemic changes must be implemented:
- Mandate Minimum Output: The National Medical Commission (NMC) should explore tying hospital accreditation (NABH) and insurance empanelment to a mandatory minimum threshold of peer-reviewed publications or registered clinical trials.
- Tax Incentives for R&D: Government frameworks should offer corporate tax breaks specifically for revenue allocated to dedicated “Academic Clinical Research Wings” within private hospitals, separating research funding from commercial clinical billing.
- National Data Trusts: Create secure, AI-driven, anonymized central data repositories where private networks can securely deposit clinical data, allowing accredited academic institutions to access it for public health breakthroughs under strict privacy laws.
- Incentivize Collaborative Trials: The Indian Council of Medical Research (ICMR) should design grant structures that explicitly require public-private partnerships, encouraging government medical colleges and corporate hospital chains to collaborate on multi-centric clinical trials.
Conclusion
India’s private healthcare sector is an absolute marvel of accessibility and clinical skill. However, that marvel is currently a house built without a library. Evidence shows that institutions producing high-quality research inherently provide better patient care. If India can successfully convert its massive 60% patient load into a corresponding research contribution, it will stop merely treating patients in the dark—it will start writing the textbooks for the rest of the world.
Sources:
- Study: Five-year analysis of research output at Indian hospitals (January 2021 – December 2025).
- Journal: Journal of Medical Evidence (Published by the BMJ Group).
- Lead Authors: Dr. Samiran Nundy and Dr. Paramanand Tiwari (Sir Ganga Ram Hospital, New Delhi).
- Key Metrics Documented:
- Private hospitals handle ~60% of patients but institutions without attached medical colleges average fewer than 10 papers per year.
- The top 50 Indian private hospitals without medical colleges produced 242 publications over the 5-year period, compared to 1,530 from the top 50 with medical colleges.
- Top global institutional outputs: Mayo Clinic (US) averages 8,000 papers/year; Top 10 medical colleges average 16,000+ in China, ~14,500 in the US, and 13,500 in the UK.
- India ranks 4th globally in publication quantity but drops to 9th in quality/citations.
The Author is the former Executive Director of the Indian Journal of Clinical Practice.





{kind=link}