
When drones first appeared on battlefields, military establishments reacted with dismissal. They were seen as toys, not weapons—incapable of replacing the skill of a pilot, the judgment of a commander, or the discipline of a structured force. Conventional military wisdom held that war required boots on the ground, a rigid chain of command, and the controlled application of force through established hierarchies.
When drones first appeared on battlefields, military establishments reacted with dismissal. They were seen as toys, not weapons—incapable of replacing the skill of a pilot, the judgment of a commander, or the discipline of a structured force. Conventional military wisdom held that war required boots on the ground, a rigid chain of command, and the controlled application of force through established hierarchies.
Then the drones kept appearing. Not because militaries invited them, but because non-state actors, insurgents, and eventually conventional forces realized that the old system—centralized, expensive, and slow—could be bypassed. A thousand-dollar drone could do what a million-dollar jet could not: be everywhere at once, strike with asymmetric speed, and operate entirely outside the structures built to control warfare.

Healthcare in 2026 is experiencing its drone moment. But this disruption is not powered only by technology. It is fueled by a profound and growing consumer disillusionment. In a country like India, the high-cost, provider-led system is seen by many patients not as an ally, but as a monument to institutional inertia.
The Perception Problem: High-Cost Medicine, Low-Value Results
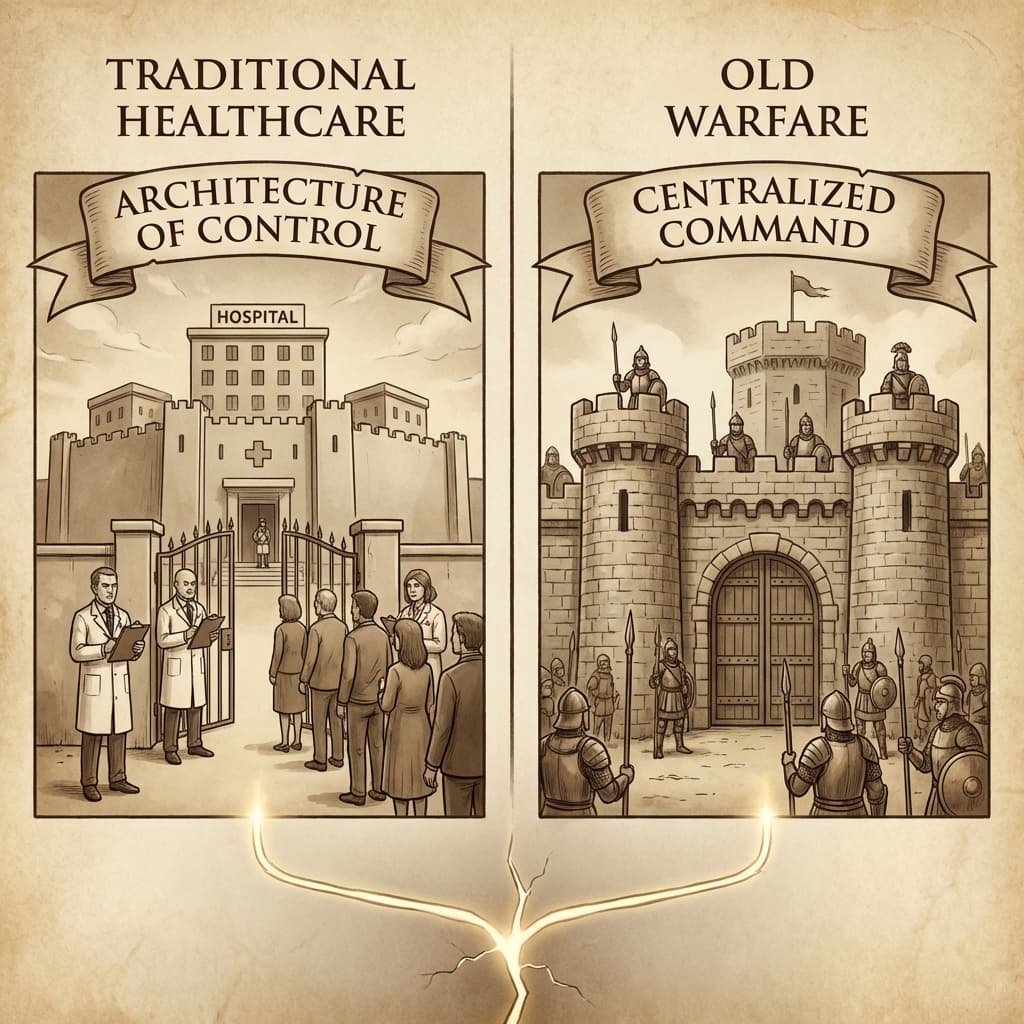
Traditional healthcare is built on an Architecture of Control. Like old warfare, it relies on centralized command (hospitals), professional gatekeepers (physicians), and a monopoly on authority (diagnosis and treatment).
Both systems assume that the complexity of the domain requires expert control and that “amateurs” cannot—should not—operate without professional supervision. Both built elaborate structures to enforce these boundaries. But as in warfare, two core assumptions are shattering this monopoly.
“Young People Are Dying”: Despite advancements in interventional cardiology, the public looks at the rising incidence of sudden heart attacks in seemingly healthy, young adults and wonders: “What is the point of the high-cost system if it can’t see this coming?”
Assumption 1: Modern Medicine can Solve the Problem. The public narrative is one of breakthrough, precision medicine, and groundbreaking drug discovery. But the perception on the ground is different.
Assumption 2: The Expert Command Structure ensures a Safe and Long Life. The structure’s failure is highly visible.
“You Cannot Reverse Diabetes”: To the patient, the modern medical establishment appears to have a single script: “We can only manage your diabetes, not reverse it.” The consumer looks at the growing arsenal of SGLT2 inhibitors and GLP-1 analogs and sees only life-long medication, a burden on their finances and their autonomy.
“Young People Are Dying”: Despite advancements in interventional cardiology, the public looks at the rising incidence of sudden heart attacks in seemingly healthy, young adults and wonders: “What is the point of the high-cost system if it can’t see this coming?”
When a patient believes that the primary function of the medical establishment is managing their decline rather than promoting their health, they will not wait for the establishment to fix itself.
When a patient believes that the primary function of the medical establishment is managing their decline rather than promoting their health, they will not wait for the establishment to fix itself
The Indian Context: A “Bypass” Prepared by History
If the drone moment revealed itself in asymmetric conflicts, India’s healthcare landscape offers a preview of global disruption. In India, patients never fully accepted the “rules” of centralized control, because the infrastructure to enforce them was incomplete.
India has long existed in what might be called a “post-prescription” reality. Despite tighter digital tracking implemented in 2025, the country remains a massive consumer of antibiotics without formal slips. The medical establishment correctly warns of Antimicrobial Resistance (AMR). Recent data from the GRAM Project (Global Research on Antimicrobial Resistance) forecasts over 39 million deaths globally between 2025 and 2050 that are directly attributable to AMR, with South Asia bearing the heaviest burden.
Yet, patients continue to bypass the gatekeepers. The reasons are structural, but also perceptional.

The Functional Shortage: While India’s doctor-population ratio has technically reached 1:811 (surpassing the WHO 1:1,000 mandate), this figure includes AYUSH practitioners and masks a severe urban-rural divide.
The High-Cost, Slow Friction: Even with the expansion of PM-JAY lowering Out-of-Pocket Expenditure (now estimated at 39.4% by the Economic Survey 2024-25), the time-cost of access remains high. A pharmacist is minutes away; a specialist is often weeks away.
The Belief Gap: If the consumer believes the specialist will only offer management (not a solution) for their heart problem or diabetes, why endure the high friction of that encounter?
The Wearable Signal and the Rise of the Asymmetric Actor
India is now the world’s largest wearable market by volume. This is not a fitness trend; it is the arming of the consumer. Low-cost wearables (a ₹1500 tracker, not an Apple Watch) are the “low-cost drones” gathering intelligence. Patients are not just asking for a diagnosis; they are executing a mission to find a better, faster, and cheaper answer.
In 2026, patients walk into pharmacies not with a prescription, but with their own data—heart rate variability, blood pressure trends, and sleep cycles—interpreted by AI assistants (the asymmetric commander on their phone). They aren’t asking for permission to take action; they are executing their own triage.

The OTC market in India is projected to hit $11.8 billion by 2030, driven by increasing self-care behavior and growing health awareness. But the real shift is in autonomy. The “non-state actor” of healthcare is using low-cost technology to seize the command authority.
The “Bypass” is complete when the patient uses a basic digital app to monitor their blood pressure, uses an AI model to analyze the data, and then consults a data-empowered pharmacist (the new “drone operator”) to adjust their medication. The expensive hospital apparatus—the Architecture of Control—has been completely circumvented.
Conclusion: The New Equilibrium
The military establishment that dismissed drones for too long became a legacy institution that lost control of its domain. The medical establishment must confront whether it will share the same fate.
The disruption does not mean the end of physicians. It means the redistribution of functions, moving from a model of Expert Control to a Distributed Network.

What will healthcare look like in 2026 and beyond?
AI-Led Triage: The default “front door” of healthcare. Patients will use AI systems to determine urgency and the appropriate level of care, redirecting routine cases.
Continuous Monitoring: Chronic disease management (diabetes, hypertension) will shift from periodic visits to continuous remote monitoring, guided by AI analysis.
The Physician as “High Command”: Doctors will focus exclusively on complex diagnostics, surgical intervention, and the ethics of care—the “fighter jets” of the system.
The Pharmacist as “Frontline Commander”: The local pharmacist is upgraded from a “dispenser” to a “data-backed clinician,” authorized by AI-integrated platforms to handle routine care.
The Implication
For a pharmaceutical or MedTech leader, this shifts the target. You are no longer solely selling a high-cost drug or device to a specialist who is authorized to prescribe or use it. You are now competing for a patient who:
Determines their own treatment trajectory based on low-cost devices and AI advice.
Uses an algorithm to choose a cheaper, AI-recommended alternative over your premium branded product.
Consults a data-empowered pharmacist (the new “drone operator”) rather than a remote physician.
Low-cost technology has not only lowered the price of entry; it has transferred the command authority to the edge. The system is not being replaced; it is being bypassed. The question for 2026 is whether healthcare institutions and corporations will adapt to this new asymmetric, disillusionment-driven reality, or become legacy monuments to a monopoly that no longer exists.
All Images are AI Generated for Illustrations Only. E&OE
APPENDIX: CREDIBLE SOURCE LEDGER (2025-2026)
This article is built on verified data from government reports, peer-reviewed journals, and market intelligence.
——————————————————————————————————————————————
CATEGORY | SOURCE / STUDY | KEY METRIC / INSIGHT
——————————————————————————————————————————————
National Economics | Economic Survey 2024-25 (Ministry of Finance, GoI) | Out-of-Pocket Expenditure (OOPE) dropped to 39.4% from 62.6% in 2015.
——————————————————————————————————————————————
Workforce Dynamics | Ministry of Health & Family Welfare (Dec 2025 Data) | India’s official doctor-population ratio is 1:811 (includes Allopathic & AYUSH).
——————————————————————————————————————————————
AMR Global Crisis | GRAM Project / The Lancet (2024-2025 Estimate) | 39 million deaths directly attributable to AMR projected by 2050; South Asia has highest mortality rate.
——————————————————————————————————————————————
Market Evolution | Mordor Intelligence / IDC Tracker (2026 Projection) | India Smart Wearable Market valued at $3.62B in 2026; Chronic disease monitoring growing at 23.9% CAGR. India is #1 globally by volume.
——————————————————————————————————————————————
Public Sentiment | NITI Aayog Health Index (2025) / Consumer Perception Surveys (2025) | Growing consumer skepticism on “reversibility” claims for metabolic diseases and public alarm over sudden cardiac mortality in youth.
——————————————————————————————————————————————
Pharmacy Data | BMJ Open (2020 Mystery Client Study) / Updated Pharmacist Surveys (2025) | Although digitally tracked, antibiotic dispensing without a prescription still exceeds 70% in the informal sector.
——————————————————————————————————————————————
Disclaimer: This article is for informational purposes. Data reflects projections and reports available as of early 2026.



{kind=link}