

India’s caesarean section debate is drifting toward polarisation.
On one side: alarm over rising surgical deliveries.
On the other: defensive reactions to what many clinicians see as unfair vilification.
Both concerns contain truth. Neither captures the whole picture.
A C-section is one of modern medicine’s most important life-saving procedures. But when performed without clear medical indication in low-risk pregnancies, it bypasses certain physiological processes that vaginal birth naturally triggers. The mature conversation lies in understanding both realities.

The Data: A Structural Gap
According to the National Family Health Survey (NFHS-5, 2019–21):
• India overall: ~21.5%
• Public facilities: ~14–15%
• Private facilities: ~47%
The World Health Organization notes that population-level C-section rates above 10–15% are not associated with additional mortality reduction. This is not a prohibition — but it is a signal for review.
India’s national rate aligns with global averages. The divergence lies within the private sector. That divergence deserves examination — but not hysteria.
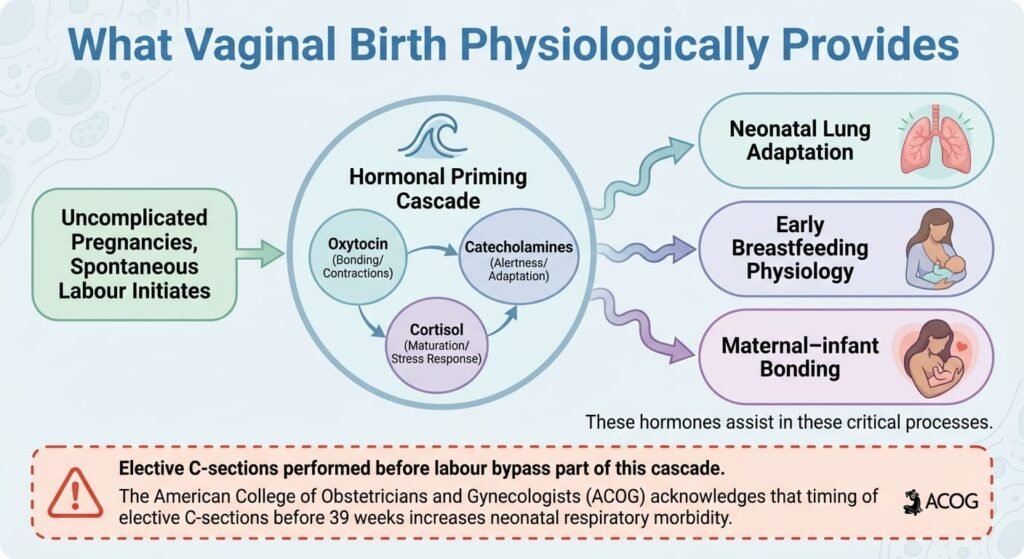
What Vaginal Birth Physiologically Provides
In uncomplicated pregnancies, spontaneous labour initiates a coordinated biological cascade.
1️⃣ Hormonal Priming
Labour triggers surges of:
• Oxytocin
• Catecholamines
• Cortisol
These hormones assist:
• Neonatal lung adaptation
• Early breastfeeding physiology
• Maternal–infant bonding
Elective C-sections performed before labour bypass part of this cascade.
The American College of Obstetricians and Gynecologists (ACOG) acknowledges that timing of elective C-sections before 39 weeks increases neonatal respiratory morbidity.
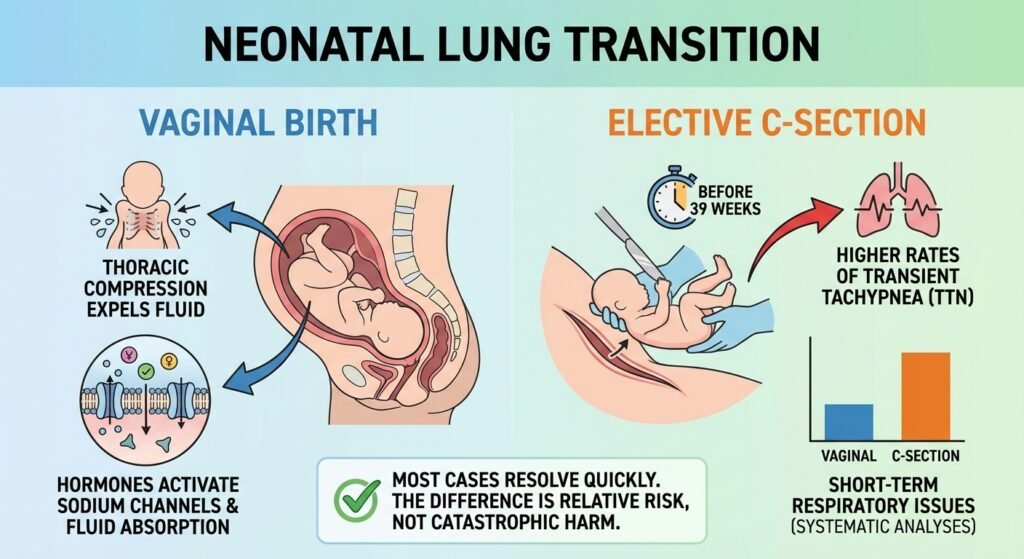
2️⃣ Neonatal Lung Transition
During vaginal birth:
• Thoracic compression helps expel lung fluid
• Labour hormones activate sodium channels aiding fluid absorption
Elective C-sections — particularly before 39 weeks — show higher rates of transient tachypnea of the newborn (TTN).
Systematic analyses, including work published in The Lancet, confirm higher short-term respiratory adaptation issues in planned pre-labour C-sections compared with vaginal births.
Most cases resolve quickly. The difference is relative risk, not catastrophic harm.
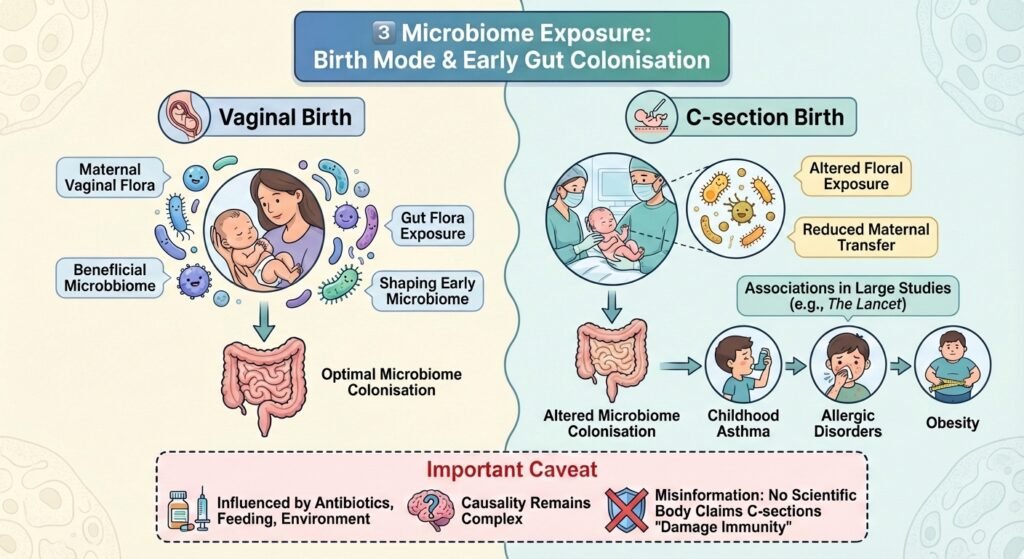
3️⃣ Microbiome Exposure
Vaginal birth exposes newborns to maternal vaginal and gut flora, shaping early microbiome colonisation.
Large epidemiological studies summarized in The Lancet have found associations between C-section birth and increased risks of:
• Childhood asthma
• Allergic disorders
• Obesity
Important caveat:
These are associations influenced by antibiotics, feeding practices, and environment. Causality remains complex.
No serious scientific body claims C-sections “damage immunity.” That is misinformation.
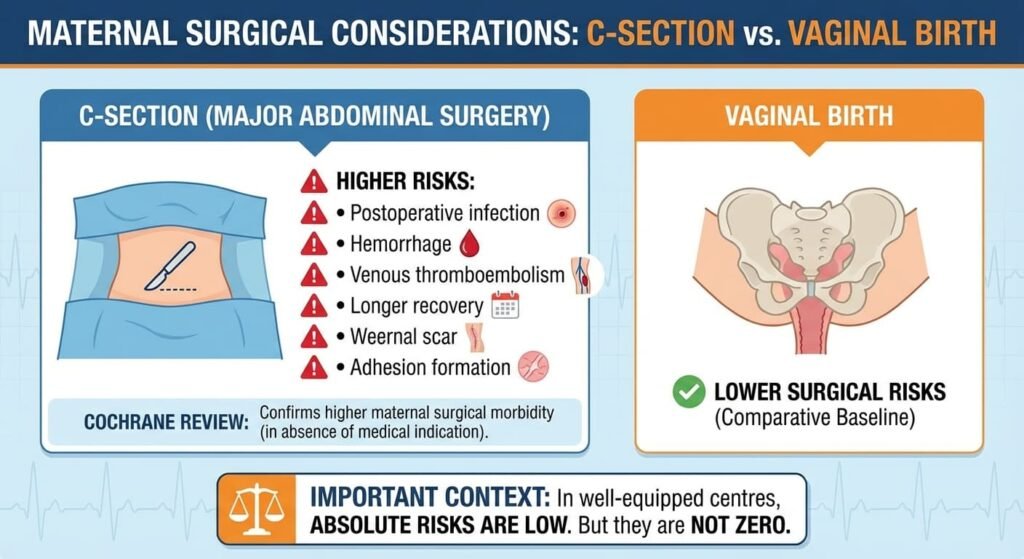
4️⃣ Maternal Surgical Considerations
C-section is major abdominal surgery.
Compared to vaginal birth, it carries higher risks of:
• Postoperative infection
• Hemorrhage
• Venous thromboembolism
• Longer recovery
• Adhesion formation
A comprehensive Cochrane review comparing planned C-section versus planned vaginal birth confirms higher maternal surgical morbidity in the absence of medical indication.
Again — in well-equipped centres, absolute risks are low. But they are not zero.
5️⃣ Future Pregnancy Implications
Repeat C-sections increase risk of:
• Placenta previa
• Placenta accreta spectrum
• Uterine rupture
• Surgical complexity
The WHO and multiple meta-analyses in The Lancet highlight rising placenta accreta risk with multiple prior C-sections.
In India’s emerging single-child urban model, this risk may be deprioritised — but clinically, it remains relevant.
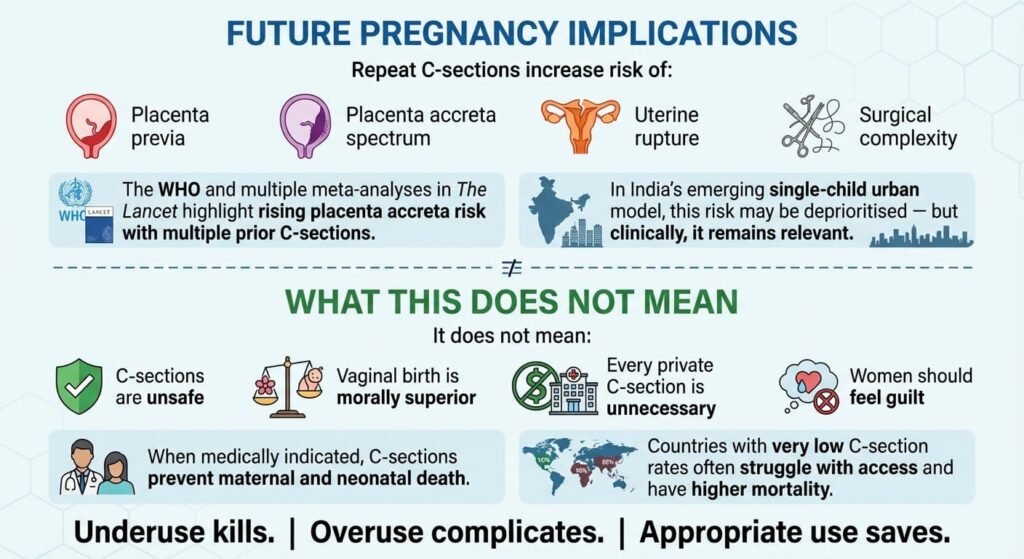
What This Does Not Mean
• C-sections are unsafe
• Vaginal birth is morally superior
• Every private C-section is unnecessary
• Women should feel guilt
When medically indicated, C-sections prevent maternal and neonatal death. Countries with very low C-section rates often struggle with access and have higher mortality.
Underuse kills.
Overuse complicates.
Appropriate use saves.
The Real Reform Conversation: The debate must move from emotion to optimisation.
Policy should focus on:
• Risk-adjusted hospital-level reporting
• Strict adherence to 39-week elective timing
• Insurance neutrality
• Strengthening midwife-led labour models
• Transparent documentation
Healthcare systems follow incentive design. Align the system, and utilisation patterns recalibrate naturally.
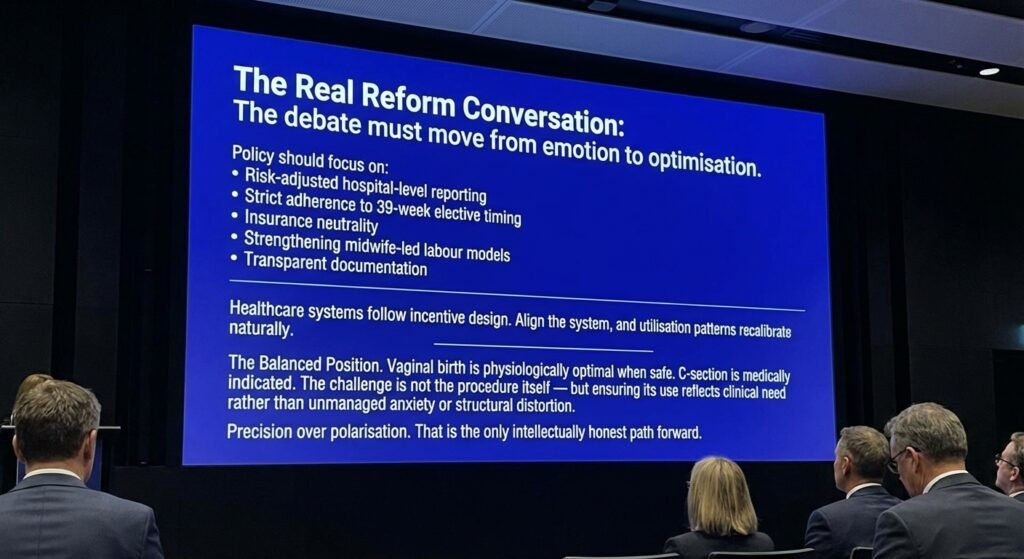
The Balanced Position. Vaginal birth is physiologically optimal when safe. C-section is medically optimal when indicated.
The challenge is not the procedure itself — but ensuring its use reflects clinical need rather than unmanaged anxiety or structural distortion.
Precision over polarisation. That is the only intellectually honest path forward.

All Images are AI Generated for Illustration Only. E&OE
Sources
1. World Health Organization
• WHO Statement on Caesarean Section Rates (2015)
• WHO Global C-section Estimates (2018, 2021 updates)
2. National Family Health Survey (NFHS-5, 2019–21)
• Ministry of Health & Family Welfare, Government of India
3. American College of Obstetricians and Gynecologists
• Committee Opinion on Avoidance of Nonmedically Indicated Early-Term Deliveries
• Clinical guidance on timing of elective C-sections
4. The Lancet
• Betrán AP et al., 2021 – Global C-section trends
• Boerma T et al., 2018 – Worldwide epidemiology
• Studies on long-term child health associations
5. Cochrane
• Reviews comparing planned C-section vs planned vaginal birth





{kind=link}