Indian healthcare is sometimes an enigma: on one hand is the finest center of medical excellence, while on the other, public health issues still lag. Apart from the highest incidence of diabetes on the chronic side, and Tuberculosis on the infectious disease side, as per NFHS data, more than 50% of women in India suffer from Anemia. That is every second woman across rural and urban areas.
In your personal surroundings, how many women can you recall actively dealing with their health issues? Doctors across specialties will tell you that women in India prioritize their families over their personal well-being and health. Similar will be the case for men above 50 with family responsibilities. But imagine, most healthcare communication is directed at men and women, who are more focused on the family than themselves. Does it call for a rethinking on whom should the messaging focus?

Rethinking the role of institutions
Imagine a public hospital. What are the images that prop up in your mind: crowds, chaos, queues! Rewind, think again. It is not just the patient. There are near and dear ones accompanying the patient. Like the patient is in pain, the caregiver is also enduring hardships: this is an invisible stakeholder in the Indian healthcare ecosystem. A recent study by AIIMS Patna, highlighted that mental distress among caregivers of cancer patients is a reality, but often overlooked Link.
Cultural theorists will explain this phenomenon as a low-context society; fatalistic; strong family ties; community relationships being important, etc. Economics experts will consider it more compulsion of accessibility and affordability, than a cultural mooring. Dig deeper, every nation in the world suffers from discrepancies in its healthcare system.
Like every country’s healthcare system is different and unique, so is the socio-cultural context of the patients and healthcare providers. In developed economies, with regimented systems for doctors’ access, the timelines for doctor appointments are stretched. In India, doctors are easily accessible, especially in public health units (making it one of the risks for violence against doctors). The same invisible caregiver mentioned above becomes a preparator of violence against the care-provider medical staff in hospitals!
In a private hospital in suburban Mumbai, managed by a religious sect, the doctor addresses a senior nurse as ‘Mataji’ (mother/ revered). Every morning, in the reception area, a monk delivers a sermon on matters of life, happiness, pain, etc. without any religious connotations: people from diverse communities sit listening in rapt attention. The front office staff at the billing counter politely attends to queries and the whole approach is to help the attendee. This is a very different experience than any other hospital in the city. Whether this hospital also faces patient or caregiver ire is a matter of study.
One of India’s best hospitals and medical colleges, located in Southern India, has its religious identity in the name itself. It is a center of excellence across specialties; some of the finest doctors come from this institute and its alumni put the institution’s name on personal profiles as a badge of honor. It attracts patients not just from its city and state, but from other states, hundreds of kilometers away.
These examples indicate that healthcare can be a great unifying force. Does it call for a rethinking of how healthcare institutions see their role in wellness, and not just treating diseases? Something similar, along the lines of WHO’s definition of health – not mere absence of disease – but complete well-being, including for the caregiver accompanying the patient!
Rethinking the role of every Individual in the healthcare ecosystem
A common patient grouse in India is the lack of time Doctors spend explaining details. A look at the sheer volume of patients in health setups perhaps answers this gap. Many times, other stakeholders rise to the occasion for providing information, like patient support groups. Recently, there was an unusual experience of such support. On a visit to a public hospital, I noticed this patient finding it difficult to understand from the Resident Doctor, where to get the prescribed medicine. A medical representative sitting close by, waiting for a doctor, walked up to him and explained the process, making it easier for the patient to shorten the process of getting medicines (mind you, it was the free drugs provided in public hospitals and the medical representative had nothing to benefit).

This single incident left at least two people carrying back positive perceptions about the medical representative – the patient and this researcher. It was a moment of truth for us, not just about the individual who helped, but the entire community of medical representatives. It also triggered a thought: could this vast force of medical representatives be necessary ‘information champions’ in public health emergencies or pandemics? Well-informed, disciplined professionals, who interact with doctors for medical information, will find providing accurate medical information a natural calling. A force of a hundred thousand medical reps is a force multiplier for the outreach of the right health messaging, impacting millions of households and lives! The time now for rethinking and calling each stakeholder of the healthcare ecosystem for their contribution towards the larger well-being!
Another invisible stakeholder of the healthcare ecosystem
Who was an important pillar of India’s fight against the COVID pandemic? The medical students. Working tirelessly, theirs is a story of grit and persistence. Twitter was full of their personal sagas about ward duties, deaths around, and the despicable but necessary covid protection gear that they had to wear throughout the day. Mind you, it was these young doctors who were holding fort as many seniors could not attend due to age-related restrictions or having co-morbidities.
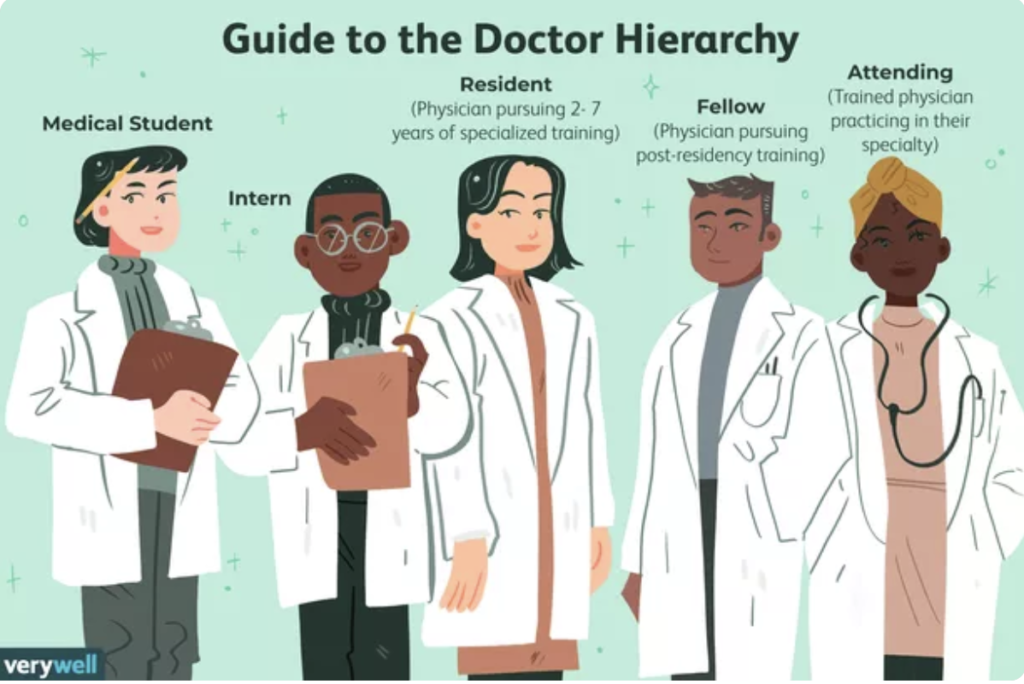
In all the noise about ‘healthcare warriors,’ this young lot didn’t get the credit they deserved. These are the same young doctors who face violence at duty, that we keep hearing and reading about. How violence impacts the thinking and behavior of medical students who face it, is a future research area for me.
Where to begin
Many years back, Each One, Teach One, was an educational initiative in India to improve literacy levels. The individual is at the core of any change or new thinking. The change agenda for healthcare communications should begin with a realization across the healthcare system and individuals on their role with a single focus – ‘change begins with ‘me’.
Noumaan Qureshi is pursuing his PhD in communications and has two decades of work experience in healthcare communications.